

Volume 5, Issue 1 (June 2019)
Elderly Health Journal 2019, 5(1): 19-31 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Zamri N A A, Harith S, Yusoff N A M, Hassan N M, Qian Ong Y. Prevalence, Risk Factors and Primary Prevention of Osteoarthritis in Asia: A Scoping Review. Elderly Health Journal 2019; 5 (1) :19-31
URL: http://ehj.ssu.ac.ir/article-1-132-en.html
URL: http://ehj.ssu.ac.ir/article-1-132-en.html
Nur Aimi Asyrani Zamri 
 , Sakinah Harith *
, Sakinah Harith *  , Noor Aini Mohd Yusoff , Nurulhuda Mat Hassan , Ying Qian Ong
, Noor Aini Mohd Yusoff , Nurulhuda Mat Hassan , Ying Qian Ong
, Sakinah Harith * , Noor Aini Mohd Yusoff , Nurulhuda Mat Hassan , Ying Qian Ong
School of Nutrition and Dietetics, Faculty of Health Sciences, Universiti Sultan Zainal Abidin, Gong Badak Campus, Kuala Nerus, Terengganu, Malaysia , sakinahharith@unisza.edu.my
Full-Text [PDF 375 kb]
(5389 Downloads)
| Abstract (HTML) (4876 Views)
Table 1. Key terms in the scoping review
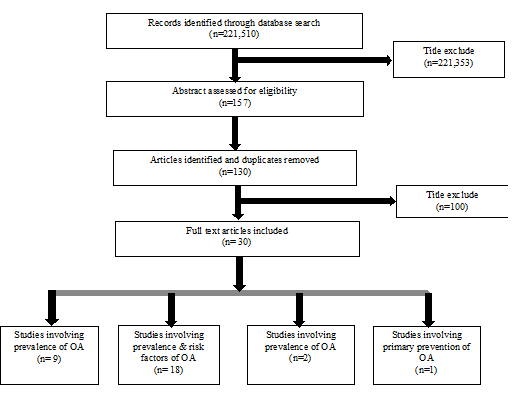
Figure 1. Flow chart of scoping review (based on framework by Arksey & OˋMalley, 2005)
Full-Text: (2851 Views)
Prevalence, Risk Factors and Primary Prevention of Osteoarthritis in Asia: A Scoping Review
Nur Aimi Asyrani Zamri 1, Sakinah Harith 1*, Noor Aini Mohd Yusoff 1, Nurulhuda Mat Hassan 2, Ying Qian Ong 1
1. School of Nutrition and Dietetics, Faculty of Health Sciences, Universiti Sultan Zainal Abidin, Gong Badak Campus, Kuala Nerus, Terengganu, Malaysia
2. Faculty of Medicine, Universiti Sultan Zainal Abidin, Medical Campus, Kuala Terengganu, Terengganu, Malaysia
Article history
Received 21 Nov 2018
Accepted 14 May 2019
A B S T R A C T
Introduction: Osteoarthritis (OA) is estimated to be the eleventh leading cause of disability worldwide. In Asian countries, OA is much less well-known than in the caucasian population and strongly associated with aging. Therefore, this article focuses comprehensively on the prevalence, risk factors and primary prevention for OA identified in Asian countries.
Methods: This scoping review used the methodological framework by Arksey and O'Malley (2005). Pertaining to this topic, a comprehensive search on academic journals published from 2008 to 2018 (English) was conducted.
Results: A total of 30 studies were selected in this review from 221,510 studies screened from electronic databases. The overall prevalence of OA is in a range of 20.5% to 68.0%. Most of the Asian populations reported to have knee OA in a range of 13.1% to 71.1% in various Asian countries. Risk factors that have been associated with OA are advanced age, being the female and obesity. Osteoporosis, higher body mass density, low level of education, family history of OA, smoking and environmental factors appeared as significant risk factors for OA. A strategic method of primary prevention for OA through lifestyle modification is reducing obesity and treating concomitant cardiovascular disease.
Conclusion: Determining OA prevalence and risk factors will provide important information for planning future cost-effective preventive strategies.
Nur Aimi Asyrani Zamri 1, Sakinah Harith 1*, Noor Aini Mohd Yusoff 1, Nurulhuda Mat Hassan 2, Ying Qian Ong 1
1. School of Nutrition and Dietetics, Faculty of Health Sciences, Universiti Sultan Zainal Abidin, Gong Badak Campus, Kuala Nerus, Terengganu, Malaysia
2. Faculty of Medicine, Universiti Sultan Zainal Abidin, Medical Campus, Kuala Terengganu, Terengganu, Malaysia
Article history
Received 21 Nov 2018
Accepted 14 May 2019
A B S T R A C T
Introduction: Osteoarthritis (OA) is estimated to be the eleventh leading cause of disability worldwide. In Asian countries, OA is much less well-known than in the caucasian population and strongly associated with aging. Therefore, this article focuses comprehensively on the prevalence, risk factors and primary prevention for OA identified in Asian countries.
Methods: This scoping review used the methodological framework by Arksey and O'Malley (2005). Pertaining to this topic, a comprehensive search on academic journals published from 2008 to 2018 (English) was conducted.
Results: A total of 30 studies were selected in this review from 221,510 studies screened from electronic databases. The overall prevalence of OA is in a range of 20.5% to 68.0%. Most of the Asian populations reported to have knee OA in a range of 13.1% to 71.1% in various Asian countries. Risk factors that have been associated with OA are advanced age, being the female and obesity. Osteoporosis, higher body mass density, low level of education, family history of OA, smoking and environmental factors appeared as significant risk factors for OA. A strategic method of primary prevention for OA through lifestyle modification is reducing obesity and treating concomitant cardiovascular disease.
Conclusion: Determining OA prevalence and risk factors will provide important information for planning future cost-effective preventive strategies.
Keywords: Osteoarthritis, Prevalence, Risk Factors, Primary Prevention
Copyright © 2019 Elderly Health Journal. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/) which permits copy and redistribute the material just in noncommercial usages, provided the original work is properly cite.
Introduction
Osteoarthritis (OA) is one of the most prevalent forms of arthritis. Research demonstrated that OA is an inflammatory disease which affect the entire synovial joint and exhibit multiple phenotypes (1). OA can be characterized by two main features. The first features of OA are progressive damage of articular cartilage, bone remodeling and new bone formation, while the second features are when synovial inflammation and fibrosis of ligaments, tendons, menisci and capsules occur in the body (2).
Introduction
Osteoarthritis (OA) is one of the most prevalent forms of arthritis. Research demonstrated that OA is an inflammatory disease which affect the entire synovial joint and exhibit multiple phenotypes (1). OA can be characterized by two main features. The first features of OA are progressive damage of articular cartilage, bone remodeling and new bone formation, while the second features are when synovial inflammation and fibrosis of ligaments, tendons, menisci and capsules occur in the body (2).
Worldwide, OA is the leading cause of chronic disability in individuals older than 70 years and has been designated a ‘priority disease’ by the World Health Organization (WHO). OA is one of the ten most disabling diseases in developed countries. In a study by Global Burden of Disease (2010), hip and knee OA were ranked as the eleventh highest contributor to global disability (3). According to WHO, it is estimated worldwide that there are 9.6% of men and 18.0% of women aged over 60 years with symptomatic osteoarthritis. Approximately 80% of people with osteoarthritis will have limitations in movement and 25% cannot perform their major daily activities (4).
Prevalence of OA is increasing because of the growing aging of the population in developed and developing countries as well as increase in risk factors leading to OA (5). OA is strongly associated with aging and Asian countries are aging rapidly. Asian elderly aged ≥ 65 years old had increased from 7% in 2008 and is predicted to achieve 16% in 2040 (6). Next, another important risk factor is obesity. Its prevalence is less but its incidence is on the rise. Therefore, it is necessary to identify the region-specific OA prevalence and examine related risk factors in order to obtain useful planning information on the future cost-effective preventive approaches and healthcare services (7).
After a thorough search for the relevant literature, it was ascertained that there is relatively limited evidence concerning characteristics of OA in Asian populations. Therefore, this review comprehensively focused on updated evidence on prevalence, risk factors and primary prevention for OA identified in Asian countries which included China, Bangladesh, India, Indonesia, Iran, Japan, Korea, Lebanon, Malaysia, Turkey and Vietnam.
Methods
A scoping review was conducted to outline the prevalence, risk factors and primary prevention of osteoarthritis in Asian countries, specifically China, Bangladesh, India, Indonesia, Iran, Japan, Korea, Lebanon, Malaysia, Turkey and Vietnam. The methodological framework proposed by Arksey and O’Malley was used to conduct this scoping review, which comprised of five stages, (1) identifying the research questions, (2) identifying relevant studies, (3) study selection, (4) charting the data and (5) collating, summarising and reporting the results (8). A flow diagram according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2009) depicted the flow of articles from search to its final selection (9).
Identifying the research questions
The review questions were: (i)What is the prevalence of osteoarthritis in Asian countries?; (ii) What are the risk factors associated with osteoarthritis?; and (iii) What is the primary prevention of osteoarthritis?
Identifying relevant studies
The search was conducted in an electronic database (MEDLINE Complete at EBSCOhost, PubMed, ScienceDirect, Scopus and Google Scholar). Relevant research websites such as WHO and Centers for Disease Control Prevention (CDC) were considered. A comprehensive search of academic journals (English) published on this topic from 2008 to 2018 was conducted. All types of studies, except systematic reviews or review papers, were included in the search. The inclusion criteria were applied to Asian countries. Titles, abstract and keywords for eligibility were examined independently by the researcher. Key terms used in the search for articles are listed in table 1.
Study selection
The reviewed studies were selected if the information about: (i) Asian countries; (ii) profile of participants; (iii) prevalence of OA; risk factor or risk factors associated with OA; and (v) primary prevention of OA, were provided.
Charting the data
The country(s), author(s), years of publication, type(s) and purpose(s) of study, sample data, and findings on prevalence, risk factors, and primary prevention of osteoarthritis relating to Asian countries are summarised in table 2.
Collating, summarising and reporting the results
Evaluations of the review on prevalence, risk factors and primary prevention of OA are illustrated in table 2.
Prevalence of OA is increasing because of the growing aging of the population in developed and developing countries as well as increase in risk factors leading to OA (5). OA is strongly associated with aging and Asian countries are aging rapidly. Asian elderly aged ≥ 65 years old had increased from 7% in 2008 and is predicted to achieve 16% in 2040 (6). Next, another important risk factor is obesity. Its prevalence is less but its incidence is on the rise. Therefore, it is necessary to identify the region-specific OA prevalence and examine related risk factors in order to obtain useful planning information on the future cost-effective preventive approaches and healthcare services (7).
After a thorough search for the relevant literature, it was ascertained that there is relatively limited evidence concerning characteristics of OA in Asian populations. Therefore, this review comprehensively focused on updated evidence on prevalence, risk factors and primary prevention for OA identified in Asian countries which included China, Bangladesh, India, Indonesia, Iran, Japan, Korea, Lebanon, Malaysia, Turkey and Vietnam.
Methods
A scoping review was conducted to outline the prevalence, risk factors and primary prevention of osteoarthritis in Asian countries, specifically China, Bangladesh, India, Indonesia, Iran, Japan, Korea, Lebanon, Malaysia, Turkey and Vietnam. The methodological framework proposed by Arksey and O’Malley was used to conduct this scoping review, which comprised of five stages, (1) identifying the research questions, (2) identifying relevant studies, (3) study selection, (4) charting the data and (5) collating, summarising and reporting the results (8). A flow diagram according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2009) depicted the flow of articles from search to its final selection (9).
Identifying the research questions
The review questions were: (i)What is the prevalence of osteoarthritis in Asian countries?; (ii) What are the risk factors associated with osteoarthritis?; and (iii) What is the primary prevention of osteoarthritis?
Identifying relevant studies
The search was conducted in an electronic database (MEDLINE Complete at EBSCOhost, PubMed, ScienceDirect, Scopus and Google Scholar). Relevant research websites such as WHO and Centers for Disease Control Prevention (CDC) were considered. A comprehensive search of academic journals (English) published on this topic from 2008 to 2018 was conducted. All types of studies, except systematic reviews or review papers, were included in the search. The inclusion criteria were applied to Asian countries. Titles, abstract and keywords for eligibility were examined independently by the researcher. Key terms used in the search for articles are listed in table 1.
Study selection
The reviewed studies were selected if the information about: (i) Asian countries; (ii) profile of participants; (iii) prevalence of OA; risk factor or risk factors associated with OA; and (v) primary prevention of OA, were provided.
Charting the data
The country(s), author(s), years of publication, type(s) and purpose(s) of study, sample data, and findings on prevalence, risk factors, and primary prevention of osteoarthritis relating to Asian countries are summarised in table 2.
Collating, summarising and reporting the results
Evaluations of the review on prevalence, risk factors and primary prevention of OA are illustrated in table 2.
Table 1. Key terms in the scoping review
| Key Search Terms |
| Osteoarthritis OR degenerative arthritis OR knee osteoarthritis AND prevalence OR incidence AND risk factor OR risk factors AND primary prevention OR primordial prevention |
| Osteoarthritis OR degenerative arthritis OR knee osteoarthritis AND occurrence OR epidemiology OR frequency AND risk factor OR risk factors AND primary prevention OR primordial prevention |
| Osteoarthritis OR hip osteoarthritis OR spine osteoarthritis OR hand osteoarthritis AND prevalence OR incidence AND risk factor OR risk factors AND primary prevention OR primordial prevention |
| Osteoarthritis OR hip osteoarthritis OR spine osteoarthritis OR hand osteoarthritis AND occurrence OR epidemiology OR frequency AND risk factor OR risk factors AND primary prevention OR primordial prevention |
Results
A total of 221, 510 titles were identified during the search. As shown in Figure 1, 30 articles were selected and included in this review. The majority of these researches are cross-sectional studies (18 studies (60%)) with 11 prospective cohort studies and 1 case
control study. The sample size in the studies ranged from 47 to 19,786 participants, aged 15 to 99 years old. This article summarizes the prevalence, risk factors and primary prevention of OA, especially in Asian countries as outlined in table 2.
A total of 221, 510 titles were identified during the search. As shown in Figure 1, 30 articles were selected and included in this review. The majority of these researches are cross-sectional studies (18 studies (60%)) with 11 prospective cohort studies and 1 case
control study. The sample size in the studies ranged from 47 to 19,786 participants, aged 15 to 99 years old. This article summarizes the prevalence, risk factors and primary prevention of OA, especially in Asian countries as outlined in table 2.
Figure 1. Flow chart of scoping review (based on framework by Arksey & OˋMalley, 2005)
Table 2. Prevalence, risk factors and primary prevention associated with OA
| Country | Study | Type & Purpose of study | Participant Characteristics | Prevalence | Risk factors | Primary prevention | ||
|---|---|---|---|---|---|---|---|---|
| India | Venkatachalam et al., 2018 |
Cross-sectional study
|
Respondents; n=1986 who living in rural area; Male: 36.6% Female: 63.4% |
Prevalence of KOA among respondents was 27.1% | Age more than 50 years, female gender, illiteracy, lower socioeconomic class, positive family history of OA, tobacco usage, diabetes and hypertension were found to be associated with KOA | No findings | ||
| Korea | Yoo, Kim, & Kim, 2018 |
Prospective cohort study
|
Participants; n=322 Aged: ≥ 50 years Median age: 71.0 years Male:46.6% Female:53.4% |
Incidence of RKOA was 10.2% (9.3% in male and 11% in female) Progression of RKOA was 13.4% (3.33% in male and 22.09% in female) Worsening of RKOA was 39.1% (29.3% in male and 47.7% in female) |
Women were significantly associated with the progression of RKOA. Being female and having a lower level of education were significantly associated with worsening of RKOA |
No findings | ||
| China | Lian et al., 2018 |
Cross-sectional study
|
Subjects; n=1446 Male: 34.6% Female: 65.4% |
Hand OA and KOA detection rate were 33.3% and 56.6% respectively | No findings | No findings | ||
| Bangladesh | Jahan, Sima, Khalil, Sohel, & Kawsar, 2017 |
Cross-sectional study
|
Samples; n=200 of OA patients Male: 43% Female:57% |
The prevalence of patients highly suffers from OA was 68% which aged 45-64 years old | No findings | No findings | ||
| Indonesia | Destianti, Fatimah, & Dewi, 2017 |
Cross-sectional study
|
KOA; n=47; Age range: 40-70 years old; Male: 10.6% Female: 89.4% |
No findings | Risk factors for KOA were passive smoker, high BMI, History of repeated use of knee joints, and family history of OA |
No findings | ||
| Iran | Kolahi et al., 2017 |
Cross-sectional study
|
Subjects; n= 952 Age range: 35-70 years old |
Out of these, 299 subjects (31.4%) had musculoskeletal disorders. OA most common rheumatic disease (53.2%) and knee most common region affected (47.7%) |
No findings | No findings | ||
|
India
|
Pal, Singh, Chaturvedi, Pruthi, & Vij, 2016 |
Cross-sectional study
|
Participants; n=5000; across five site in India; age range: above 40 years old |
Prevalence of KOA was 28.7%
KOA more prevalent in females (31.6%) than in males (28.1%)
|
Female gender, obesity and sedentary work were associated factors of KOA | No findings | ||
| China | Tang et al., 2016 |
Longitudinal cohort study
|
Participants; n=17 128; aged:45 years old and above; mean age: 59.8 years Male: 48.8% female: 51.2% |
Prevalence of SOA was 8.1% SOA more common in female (10.3%) than men ( 5.7%) |
No findings | No findings | ||
| China | Zhang et al., 2016 |
Cross-sectional study
|
Participants; n=7126; Age range: 16-90 years old; average age; 43.9±16.6 years; male: 50.6% female: 49.4% |
|
Advanced age, a sweet tooth, poor home ventilation, poor home heating, separation, divorce or death of partner, low grade occupation, low educational level. high BMI and presence of concomitant CVD were significantly associated with the presence of OA |
No findings | ||
| China | Liu et al., 2016 |
Cross-sectional community study
|
Subjects; n=3428 Age range: 40-74years old Mean age: 55±10years Men:48.5% Women:51.5% |
Prevalence of KOA was 16.57% (15.79% in women and 17.40% in men) | Aging, obesity, frequent walking, low income and relevant multiple metabolic disorders were associated factors for KOA. | No findings | ||
| Korea | Lee at al., 2015 |
Cross-sectional study
|
Subjects; n=1670; age range: 65-95 years old; mean age: 72.7±5.7 years; male: 41.7% female: 58.3% |
Out of 1670 subjects, 476 subjects were diagnosed with OA (28.5%) | Age,female gender,higher BMI and osteoporosis were significant risk factors for OA |
No findings | ||
|
Korea
|
Lee & Kim, 2015 |
Cross-sectional study
|
Participants; n= 9512; aged: ≥50 years; Mean age for men: 61.5±0.18 years: mean age for women: 63.3±0.18 years men: 42.7% women: 57.3% |
Prevalence of RKOA was 33.3%
Prevalence of SRKOA was 12.4%
|
Prevalence of KOA especially SRKOA in women, was higher in regions with high prevalence of obesity | No findings | ||
| Korea | Cho, Morey, Kang, Kim, & Kim, 2015 |
Cross-sectional study
|
Subjects; n=696; age range: 65-91 years old; mean age: 72±5 years; male: 42.8% female: 57.2% |
Prevalence of radiographic OA in:
|
|
No findings | ||
| Iran | Davatchi et al., 2015 |
Cross-sectional study
|
Participants; n=19786 Aged: ≥15 years |
Prevalence of OA was 16.9%
|
No findings | No findings | ||
| Vietnam | Ho-Pham et al.,2014 |
Cross-sectional study
|
Participants; n=658; Age range: 40-98 years old; average age: 55.5 years old; male: 25.8% female: 74.2% |
Prevalence of radiographic KOA was 34.2% (n=225), with women having higher prevalence than men (35.3% vs 31.2%) | Advancing age associated with an increased risk of radiographic KOA. Greater BMI and high score number of knee complaints associated with a greater risk of KOA | No findings | ||
| Iran | Tehrani-Banihashemi et al., 2014 |
Cross-sectional study
|
Subjects; n=1192 Aged: ≥15 years old Mean age: 38.4±18.5years male: 44.9% female: 55.1% |
Among the studies population, 316 subjects (20.5%) had OA in at least one of their joints
Neck OA (2.21%)
|
No findings | No findings | ||
| Turkey | YefiL, Hepgüler, Öztürk, Çapaci, & YesiL, 2013 |
Cross-sectional study
|
Subjects; n=522 Aged: ≥40 years Average age: 53.9±8.5 years Men:25.3% Women: 74.7% |
Prevalence of adults aged ≥40 years with symptomatic:
|
No findings | No findings | ||
|
Lebanon
|
El Ayoubi et al., 2013 |
Case control study
|
Participants; n=177 (59 cases, 118 controls) Aged: 15≥ years Male:44.1% Female: 55.9% |
No findings | Obesity, overweight and area of residence were significant risk factors for KOA | No findings | ||
| Japan | Nishimura et al., 2012 |
Prospective cohort study
|
Participants; n=1223; aged: More than 65 years old; male: 448 female:775 | Prevalence of radiographic bilateral and unilateral KOA were 21.6% and 10.0% respectively | No findings | No findings | ||
| Japan | Muraki et al., 2012 |
Longitudinal cohort study
|
Subjects from ROAD study; n=2262; male: 33.7% female: 66.3% |
The rate of incidence K/L grade ≥2 RKOA:
The rate of incidence K/L grade ≥3 RKOA:
The rate of progressive KOA:
|
Female sex was a risk factor for incident K/L grade ≥2 KOA but not associated with incident K/L grade ≥3 KOA or progressive KOA | No findings | ||
| China | Jiang et al., 2012 |
Cross-sectional study
|
Subjects; n=1196 (urban; n=600, rural; n=594) age range: 40-84 years old; mean age: 62.60±8.69 years; men: 47.9% women: 52.1% |
Prevalence of SKOA was 16.05% In urban area, 61.6% of subjects had bilateral KOA, 66.9% left KOA and 65.5% right KOA. In rural area, 71.4% of subjects had bilateral KOA, 76.6% left KOA and 78.0% right KOA |
BMI, age, sex and work status might be risk factors for urban residents BMI, age and smoking habits might be risk factors for rural dwellers |
No findings | ||
| Korea | Cho et al., 2011 |
Prospective cohort study
|
Subjects; n= 696; age range:65-99 years old; mean age: 71.7±5.3 years; male: 42.8% female: 57.2% | Prevalence of radiographic OA (38.1%), severe radiographic OA (26.4%) and TKA candidates (6.5%). Proportion of bilateral KOA was 84.5% (radiographic OA), 68.5% (severe radiographic OA) and 64.4% (TKA candidates) |
Female sex, obesity and aging were found to be associated with the risk of all 3 stages of knee OA | No findings | ||
|
Korea
|
Oh et al., 2011 |
Prospective cohort study
|
Respondents; n=679; age range: 65-97 years old; mean age: 71.8±5.7years; male: 41.7% female: 58.3% |
Radiography primary OA of the shoulder (16.1%)
Secondary OA of the shoulder (1.3%)
Mild KOA (37.7%) Moderate-to-severe KOA (26.1%) |
Older age and the presence of KOA are independent determining risk factors for shoulder OA | No findings | ||
| Japan | Nishimura et al., 2011 |
Longitudinal cohort study
|
Participants; n=360 Age range: 65-89years old Mean age:71.0±4.7 years Men:33.1% (mean age 71.3±5.1 years) Women:66.9% (mean age 70.8±4.5 years) |
The rate of incidence and progression of KOA were 4.0 and 6.0% per year | Female gender and high BMI were significantly associated with the incidence of KOA and restricted knee ROM was significantly associated with KOA progression. | |||
| Korea | Kim et al., 2010 |
Prospective cohort study
|
Subjects; n=504; Age ranged: 50-89 years old; mean age: 70.2 years; male: 45.6% female: 54.4% |
Prevalence of RKOA: n=188 (37.3%)
Prevalence of SKOA: n=121 (24.2%)
Women majority of subjects:
|
|
No findings | ||
| Japan | Yoshimura et al., 2009 |
Prospective cohort study
|
Participants; n=3040; mean age: 70.3±11.0 years; men: 34.9% (mean age:71.0±10.7 years) women: 65.1% (mean age: 69.9±11.2 years) |
Prevalence of RKOA was 54.6% (42.0% in men and 61.5% in women) | Risk factors of KOA was significantly higher in mountainous area, in women, in advanced age and higher BMI | No findings |
||
Japan |
Muraki et al., 2009 |
Prospective cohort study
|
Participants; n=2282; aged: ≥60years male: 35.8% (mean age 74.7±6.1 years) female: 64.2%(mean age 74.0±6.4 years) |
Prevalence of radiographic knee OA : KL>2 (47%) KL>3 (20.6%) Prevalence of radiographic knee OA with pain: KL>2 (26.1%) KL>3(13.2%) |
Age, BMI, female sex and rural residency were risk factors for radiographic knee OA, knee pain and and their combination | No findings | ||
| China | Kang et al., 2009 |
Cross-sectional study
|
Participants; n=1025 Aged: ≥50 years Mean age: 58±8 years Men:49.3% Women:50.7% |
Prevalence of RKOA:
Prevalence of SKOA:
|
No findings | No findings | ||
| Japan | Sudo et al., 2008 |
Cross-sectional study
|
Participants; n=598 Aged: ≥65years Male:34.3% Women:65.7% |
Prevalence of RKOA was 30.0% (17.7% in men and 36.5% in women) Prevalence of SKOA was 21.2% (10.7% in men and 26.7% in women) |
Higher BMI, female sex, older age, and higher BMD were significantly associated with increased risk for RKOA | No findings | ||
| Malaysia | Arshad et al., 2008 |
Cross-sectional survey
|
200 randomly selected general practitioners (GPs) in peninsular states of Malaysia | No findings | No findings |
Pharmacological management consist of first line treatment with:
Non-pharmacological management consist of:
Referral to physiotherapy (10%)
|
||
Abbreviation: OA=Osteoarthritis KOA=Knee Osteoarthritis RKOA=Radiographic knee Osteoarthritis SKOA=Symptomatic knee Osteoarthritis
SRKOA= Symptomatic and Radiographic Knee Osteoarthritis TKA= Total Knee Arthroplasty BMI= Body Mass Index CVD= cardiovascular disease
BMD=Bone Mineral Density ROM=Range Of Motion K/L=Kellgren/Lawrence KBD=Kashin-Beck Disease
SRKOA= Symptomatic and Radiographic Knee Osteoarthritis TKA= Total Knee Arthroplasty BMI= Body Mass Index CVD= cardiovascular disease
BMD=Bone Mineral Density ROM=Range Of Motion K/L=Kellgren/Lawrence KBD=Kashin-Beck Disease
Prevalence of Osteoarthritis
27 studies in this review examined the prevalence of OA. The overall prevalence of OA is in the range of 20.5% to 68% (10–15). The prevalence of knee OA (KOA) is shown to be in the range of 13.8% to 71.1% across the Asian populations (11, 12, 14–20), and more prevalent in females than males at 31.6% and 28.1%, respectively (18). Prevalence of radiographic KOA (RKOA) is in the range of 10.0% to 54.6% (21–26), while the prevalence of symptomatic KOA (SKOA) is in the range of 8.1% to 24.2% (20, 27–29). The rate of incidence and progression of knee OA reported are 4.0% to 10.2% and 6.0% to 13.4% per year (30, 31), respectively. The rate of incidence of RKOA in men is in the range of 6.9% to 9.3%, while women in the range of 11.0% to 13.9%. Meanwhile, the rate of progression of RKOA in men is in the range of 3.3% to 17.8%, while women is 22.3% to 22.9% (31, 32). The rate of worsening of RKOA is 39.1% with 29.3% and 47.7% for men and women, respectively (31). Besides that, the prevalence of hand OA is in the range of 2.7% to 60% (12, 14, 15, 17, 22, 28). Other than that, the prevalence of spine OA is 66% (22), shoulder OA in the range of 3.0% to 16.1% (12, 22, 33) and hip OA in the range of 0.6% to 2% (12, 22, 28). The majority of OA involved knee, hand, spine and hip. Other joints are also involved but very low in number.
Risk Factors of Osteoarthritis
Unmodifiable risk factors
Age
12 studies explored the relationship between age and OA. However, the pathogenesis of age-related OA is not fully studied. The recent evidence revealed that OA development can be attributed to age-related alteration in other tissues other than articular cartilage (34).
Gender
The association with female gender was examined in 11 studies. Females had a higher risk of having KOA and hand OA, while males were associated with spine OA (22).
Genetic
Only two studies reported an association between having a family history of OA with OA occurrence. Respondents with positive family history were more likely to develop KOA (16).
Modifiable risk factors
Pathophysiological factors
Hypertension
A positive association between hypertension and OA was found in two studies (16, 29). Presence of hypertension was significantly associated with both RKOA and SKOA (29).
Diabetes
The association between diabetes and OA was reported as discovered in two studies (12, 16). The participants with diabetic patients had 2.1 times the odds of developing KOA compared with participants without diabetes (16).
Osteoporosis
Only one study reported on osteoporosis; nonetheless, it failed to demonstrate any significant association between osteoporosis and OA (13).
Presence of KOA
KOA is a significant risk factor for shoulder OA. Prevalence of shoulder OA was higher in participants with KOA (33).
Higher bone mineral density (BMD)
High BMD was significantly associated with an increased risk for RKOA. 0.1g/cm2 increment in BMD raised the risk of KOA by 53% (35).
Lifestyle factors
Obesity
A majority of the studies in this review reported the association between obesity and OA (16 studies). Obesity or high Body Mass Index (BMI) was found to be associated with KOA (20, 22, 23, 36).
Smoking
Smoking habits might be a risk factor for KOA for rural dwellers compared to urban residents (20).
Repetitive use of joints
Repetitive use of joints at work was associated with increased risk of OA (12, 19, 29, 37).
Environmental factors
Poor home ventilation and heating
Only one study discovered an association between home ventilation and heating with OA. Subjects who had lived in well ventilated homes had lower OA than those living under poorly ventilated conditions. Also, subjects who lacked heaters in their homes had a higher prevalence of OA than did others (12).
Area residence
Three studies reported on the association between area residence and OA (26, 36,38). Residents who lived in rural areas or mountainous areas were more likely to develop KOA compared to residents who lived in urban areas (26, 38).
Socioeconomic factors
Lower education
Low educational level indicates low grade occupation. Subjects with a low level of education were more likely to develop OA (12).
Separation, divorce or death
Those who were separated, divorced or widowed were more likely to have OA (12).
Primary prevention of Osteoarthritis
There is not yet a cure for OA, but it has become clear that the management of risk and predisposing factors may slow the disease progression (39). OA management consists of multidisciplinary strategies with the aim to alleviate symptoms and enhance joint functions. The management can be classified into pharmacological and non-pharmacological interventions. In this review, only one study reported on primary prevention of OA (40).
Pharmacological treatment comprises of non-steroidal anti-inflammatory drugs (NSAIDs), analgesics and their combinations which act as first line approach. The majority of general practitioners (GPs) used NSAIDs (61%), followed by analgesics (35%) and a few GPs combined both agents (4%). Non-pharmacological management was under-utilised by most GPs as only 27% advised on exercise, 33% would advise on weight reduction, while seeking for physiotherapist was the least preferred. Other than that, complementary medicines were also used for treatment such as glucosamine, chondroitin, cod liver oil and evening primrose oil (40)
Discussion
OA is the most prevalent form of rheumatic disease and the major cause of disability in Asian countries. In this review, most of the burdens of disability were attributable to the involvement of the knees. Prevalence of OA in the Asian region has kept on increasing due to the ageing population and the rising prevalence of obesity (25, 42).
OA is strongly associated with ageing and the Asian region is aging rapidly. In this review, most of the studies found that the subjects who were aged 50 years and above were more vulnerable to be affected with OA compared to the subjects below 50 years of age (13, 18, 21). A number of factors influence the aging alteration in joint tissues which can lead to OA development. These factors included the development of the senescent secretory phenotype and aging alteration in the matrix due to cell senescence which result in synthesis of advanced glycation end-products that impact the mechanical properties of joint tissues (34).
Majority of the studies in this review reported that being a female and having a high body mass index were significantly associated with knee OA (14, 19, 31) These findings were supported by Nishimura et al. who reported that not only were women more likely to have OA than men, they also have more severe OA (30). The significant prevalence of OA in women around the time of menopause has led to multiple investigations of the hormonal effect on the pathophysiology of OA. However, the results on the effect of estrogen therapy from these investigations have been conflicting as estrogen use is linked to a healthy lifestyle and osteoporosis, which can lower the risk of osteoarthritis (39). Other than that, Zhang et al. reported that having a high body mass index or obesity may cause knee or hip OA. This is because knee and hip joints that withstand long term burden will tear the synovial joint which subsequently lead to ligamentous and other structural support failure (15).
Repetitive use of joints at work is associated with increased risk of OA in almost all of the Asian region(3, 13, 30, 35). According to a research on Osteoarthritis-Osteoporosis Against Disability (ROAD) which was conducted in Japan, occupations involving squatting or kneeling for more than 2 hours per day were associated with high risk of moderate to severe radiographic knee OA. Besides that, the ROAD study also reported that Japanese people aged 60 years and above with an occupation involving climbing for more than 1 hour a day, standing more than 2 hours a day, lifting weights of 10 kg or more at least once a week and walking more than 3 km a day increased risk of radiographic knee OA(35).
High prevalence of OA highlighted the importance of primary prevention. Primary prevention involves pharmacological and non-pharmacological treatments (43). According to Zhang et al. it is important for education programmes to be specific and depend on individual needs, goals and functional capabilities. Patients with OA who have an understanding of the disease tend to cope better and reported less pain. Lifestyle modifications including dietary weight loss and physical active have shown to improve health-related quality of life among OA patients. According to the Framingham Heart Study, the women who had lost 5 kg their weight had lower the risk of symptomatic knee OA development by 50%. This is supported by the same study which reported that weight loss intervention can lower the risk of radiographic knee OA development. This intervention is also shown to be effective among knee OA by minimizing the pain and disability. Another study evaluated the effect of exercise on knee and hip OA and demonstrated an improvement in pain and function (25, 33, 42, 44).
Last but not least, the shortcoming of this scoping review is there was scarce study conducted in Asian countries on the prevalence rates, risk factors and OA primary prevention. Therefore, it is necessary that future collaborative researchers given attention to the overall prevalence rates and guidelines of primary prevention by focusing on lifestyle modification among Asian populations.
Conclusion
High prevalence of knee pain or symptomatic knee OA was observed among Asian elderly in rural and urban areas. Similar findings were also found in other regions worldwide. This issue should be given concern due to current rapid aging and raising obesity cases in most Asian countries. Besides that, simple approach or workplace practices to minimize exposure to continuous heavy manual occupational activities or long term kneeling or squatting should be developed in order to reduce the prevalence of chronic knee pain and disability among Asian population.
Conflict of interest
The author(s) declare(s) no potential conflicts of interests.
Acknowledgements
We would like to express our gratitude to those who have helped in the writing of this article.
Authors' Contribution
Nur Aimi Asyrani Z. and Sakinah H. conceived of the presented idea. Nur Aimi Asyrani Z. screened and collected the data. Sakinah H. supervised the review. Nur Aimi Asyrani Z. wrote the manuscript with support from Ying Qian O., Sakinah H. Noor Aini M.Y. and Nurulhuda M.H. provided critical feedback, shaped the review and provided technical assistance. All authors discussed the results and commented on the manuscript.
References
1. Mobasheri A, Batt M. An update on the pathophysiology of osteoarthritis. Annals of Physcal and Rehabiltation Medicine. 2016; 59(5–6): 333–9.
2. Li Y, Wei X, Zhou J, Wei L. The age-related changes in cartilage and osteoarthritis. BioMed Research International. 2013; 2013: 1-12.
3. Cross M, Smith E, Hoy D, Nolte S, Ackerman I, Fransen M, et al. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Annals of the Rheumatic Diseases. 2014; 73(7) :1323–30.
4. Wittenauer R, Smith L, Aden K. Background paper background paper 6.12 osteoarthritis. World Health Organization. 2013;1–31. Available from: http://www.who.int/medicines/areas/priority_medicines/BP6_12Osteo.pdf
5. Palazzo C, Nguyen C, Lefevre-Colau MM, Rannou F, Poiraudeau S. Risk factors and burden of osteoarthritis. Annals of Physical and Rehabilitation Medicine. 2016; 59(3): 134–8.
6. Bureau USC. An aging world : 2008. Aging. 2009. 7. Johnson VL, Hunter DJ. The epidemiology of osteoarthritis. Best Practice & Research Clinical Rheumatology. 2014; 28(1): 5–15.
8. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology. 2005; 8(1): 19–32.
9. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Medicine. 2009; 6(7):1-6.
10. Jahan I, Sima SH, Khalil M, Sohel MD, Kawsar MH. Survey on prevalence, risk factors and treatment pattern of osteoarthritis in Bangladesh: retrospective study. Rheumatology: Current Research. 2017; 7(4): 1-6.
11. Kolahi S, Khabbazi A, Malek Mahdavi A, Ghasembaglou A, Ghasembaglou A, Aminisani N, et al. Prevalence of musculoskeletal disorders in Azar cohort population in Northwest of Iran. Rheumatology International. 2017; 37(4): 495–502.
12. Zhang JF, Song LH, Wei JN, Zhang AL, Dong HY, Wen HY, et al. Prevalence of and risk factors for the occurrence of symptomatic osteoarthritis in rural regions of Shanxi Province, China. International Journal of Rheumatic Diseases. 2016; 19(8): 781–9.
13. Lee KM, Chung CY, Sung KH, Lee SY, Won SH, Kim TG, et al. Risk factors for osteoarthritis and contributing factors to current arthritic pain in south Korean older adults. Yonsei Medical Journal. 2015; 56(1): 124–31.
14. Davatchi F, Sandoughi M, Moghimi N, Jamshidi AR, Tehrani Banihashemi A, Zakeri Z, et al. Epidemiology of rheumatic diseases in Iran; Adjusted analysis of 4 copcord studies. International Journal of Rheumatic Diseases. 2016; 19(11): 1056-62.
15. Tehrani-Banihashemi A, Davatchi F, Jamshidi AR, Faezi T, Paragomi P, Barghamdi M. Prevalence of osteoarthritis in rural areas of Iran: a WHO-ILAR COPCORD study. International Journal of Rheumatic Diseases. 2014; 17(4): 384–8.
16. Venkatachalam J, Natesan M, Eswaran M, Johnson AKS, Bharath V, Singh Z. Prevalence of osteoarthritis of knee joint among adult population in a rural area of Kanchipuram District, Tamil Nadu. Indian Journal of Public Health. 2017; 62(2): 117–22.
17. Lian W, Liu H, Song Q, Liu YQ, Sun LY, Deng Q, et al. Prevalence of hand osteoarthritis and knee osteoarthritis in Kashin-Beck disease endemic areas and non Kashin-Beck disease endemic areas: A status survey. PLoS One. 2018; 13(1): 1-15.
18. Pal CP, Singh P, Chaturvedi S, Pruthi K, Vij A. Epidemiology of knee osteoarthritis in India and related factors. Indian Journal of Orthopaedics. 2016; 50(5): 518-22.
19. Liu Y, Zhang H, Liang N, Fan W, Li J, Huang Z, et al. Prevalence and associated factors of knee osteoarthritis in a rural Chinese adult population: an epidemiological survey. BMC Public Health. 2016; 16(94): 1–8.
20. Jiang L, Rong J, Zhang Q, Hu F, Zhang S, Li X, et al. Prevalence and associated factors of knee osteoarthritis in a community-based population in Heilongjiang, Northeast China. Rheumatology International. 2012; 32(5): 1189–95.
21. Lee S, Kim S-J. Prevalence of knee osteoarthritis, risk factors, and quality of life: the fifth Korean national health and nutrition examination survey. International Journal of Rheumatic Diseases. 2017; 20(7): 809–17.
22. Cho HJ, Morey V, Kang JY, Kim KW, Kim TK. Prevalence and Risk Factors of Spine, Shoulder, Hand, Hip, and Knee Osteoarthritis in Community-dwelling Koreans Older Than Age 65 Years. Clinical Orthopaedics and Related Research. 2015; 473(10): 3307–14.
23. Ho-Pham LT, Lai TQ, Mai LD, Doan MC, Pham HN, Nguyen TV. Prevalence of radiographic osteoarthritis of the knee and its relationship to self-reported pain. PLoS One. 2014; 9(4): 1–7.
24. Nishimura A, Hasegawa M, Wakabayashi H, Yoshida K, Kato K, Yamada T, et al. Prevalence and characteristics of unilateral knee osteoarthritis in a community sample of elderly Japanese: do fractures around the knee affect the pathogenesis of unilateral knee osteoarthritis?. Journal of Orthopaedic Science. 2012; 17(5): 556–61.
25. Cho HJ, Chang CB, Kim KW, Park JH, Yoo JH, Koh IJ, et al. Gender and prevalence of knee osteoarthritis types in elderly Koreans. The Journal of Arthroplasty. 2011; 26(7): 994–9.
26. Yoshimura N, Muraki S, Oka H, Mabuchi A, En-Yo Y, Yoshida M, et al. Prevalence of knee osteoarthritis, lumbar spondylosis, and osteoporosis in Japanese men and women: The research on osteoarthritis/osteoporosis against disability study. Journal of Bone and Mineral Metabolism. 2009; 27(5): 620–8.
27. Tang X, Wang S, Zhan S, Niu J, Tao K, Zhang Y, et al. The prevalence of symptomatic knee osteoarthritis in china: results from the china health and retirement longitudinal study. Arthritis & Rheumatology. 2016; 68(3): 648–53.
28. YefiL H, Hepgüler S, Öztürk C, Çapaci K, YesiL M. Prevalence of symptomatic knee, hand and hip osteoarthritis among individuals 40 years or older: a study conducted in izmir city. Acta Orthopaedica er Traumatologica Turcica. 2013; 47(4): 231–5.
29. Kim I, Kim HA, Seo Y Il, Song YW, Jeong JY, Kim DH. The prevalence of knee osteoarthritis in elderly community residents in Korea. Journal of Korean Medical Science. 2010; 25(2): 293–8.
30. Nishimura A, Hasegawa M, Kato K, Yamada T, Uchida A, Sudo A. Risk factors for the incidence and progression of radiographic osteoarthritis of the knee among Japanese. International Orthopaedics. 2011; 35(6): 839–43.
31. Yoo JJ, Kim DH, Kim HA. Risk factors for progression of radiographic knee osteoarthritis in elderly community residents in Korea. BMC Musculoskeletal Disorders. 2018; 19(1): 1–7.
32. Muraki S, Akune T, Oka H, Ishimoto Y, Nagata K, Yoshida M, et al. Incidence and risk factors for radiographic knee osteoarthritis and knee pain in Japanese men and women: a longitudinal population-based cohort study. Arthritis and Rheumatism. 2012; 64(5): 1447–56.
33. Oh JH, Chung SW, Oh CH, Kim SH, Park SJ, Kim KW, et al. The prevalence of shoulder osteoarthritis in the elderly Korean population: Association with risk factors and function. Journal of Shoulder and Elbow Surgery. 2011; 20(5): 756–63.
34. Li Y, Wei X, Zhou J, Wei L. The Age-Related Changes in Cartilage and Osteoarthritis. BioMed Resarch International. 2013; 2013: 1-12.
35. Sudo A, Miyamoto N, Horikawa K, Urawa M, Yamakawa T, Yamada T, et al. Prevalence and risk factors for knee osteoarthritis in elderly Japanese men and women. Journal of Orthopaedic Science. 2008; 13(5): 413–8.
36. El Ayoubi N, Chaaya M, Mahfoud Z, Habib R, Uthman I, Slim Z. Risk factors for incident symptomatic knee osteoarthritis: A population-based case control study in Lebanon. International Journal of Rheumatic Diseases. 2013; 16(2): 211–8.
37. Destianti NA, Fatimah SN, Dewi S. Vitamin C intake and risk factors for knee osteoarthritis. Althea Medical Journal. 2017; 4(2): 173–7.
38. Oka H, Akune T, Muraki S, En-Yo Y, Yoshida M, Saika A, et al. Association of low dietary vitamin K intake with radiographic knee osteoarthritis in the Japanese elderly population: Dietary survey in a population-based cohort of the ROAD study. Journal of Orthopaedic Science. 2009; 14(6): 687–92.
39. Muraki S, Oka H, Akune T, Mabuchi A, En-yo Y, Yoshida M, et al. Prevalence of radiographic knee osteoarthritis and its association with knee pain in the elderly of Japanese population-based cohorts: The ROAD study. Osteoarthritis and Cartilage. 2009; 17(9): 1137–43.
40. Anandacoomarasamy A, March L. Current evidence for osteoarthritis treatments. Therapeutic Advances Musculoskeletal Disease. 2010; 2(1): 17–28. 41. Anwar A, Rashid R, Gupta EDAS. A survey of the primary care management of osteoarthritis in Malaysia : a view from a rheumatologist’s perspective. International Journal of Rheumatic Diseases. 2008; 11(3): 246–50.
42. Kang X, Fransen M, Zhang Y, Li H, Ke Y, Lu M, et al. The high prevalence of knee osteoarthritis in a rural Chinese population: the Wuchuan osteoarthritis study. Arthritis and Rheumatism. 2009; 61(5): 641–7. 43. Ratzlaff CR, Liang ML. Prevention of injury related knee osteoarthritis: opportunities for the primary and secondary prevention of knee osteoarthritis. Arthritis Research & Therapy. 2010; 12(215): 1-8.
44. Takeda H, Nakagawa T, Nakamura K, Engebretsen L. Prevention and management of knee osteoarthritis and knee cartilage injury in sports. British Journal of Sports Medicine. 2011; 45(4): 304–9.
27 studies in this review examined the prevalence of OA. The overall prevalence of OA is in the range of 20.5% to 68% (10–15). The prevalence of knee OA (KOA) is shown to be in the range of 13.8% to 71.1% across the Asian populations (11, 12, 14–20), and more prevalent in females than males at 31.6% and 28.1%, respectively (18). Prevalence of radiographic KOA (RKOA) is in the range of 10.0% to 54.6% (21–26), while the prevalence of symptomatic KOA (SKOA) is in the range of 8.1% to 24.2% (20, 27–29). The rate of incidence and progression of knee OA reported are 4.0% to 10.2% and 6.0% to 13.4% per year (30, 31), respectively. The rate of incidence of RKOA in men is in the range of 6.9% to 9.3%, while women in the range of 11.0% to 13.9%. Meanwhile, the rate of progression of RKOA in men is in the range of 3.3% to 17.8%, while women is 22.3% to 22.9% (31, 32). The rate of worsening of RKOA is 39.1% with 29.3% and 47.7% for men and women, respectively (31). Besides that, the prevalence of hand OA is in the range of 2.7% to 60% (12, 14, 15, 17, 22, 28). Other than that, the prevalence of spine OA is 66% (22), shoulder OA in the range of 3.0% to 16.1% (12, 22, 33) and hip OA in the range of 0.6% to 2% (12, 22, 28). The majority of OA involved knee, hand, spine and hip. Other joints are also involved but very low in number.
Risk Factors of Osteoarthritis
Unmodifiable risk factors
Age
12 studies explored the relationship between age and OA. However, the pathogenesis of age-related OA is not fully studied. The recent evidence revealed that OA development can be attributed to age-related alteration in other tissues other than articular cartilage (34).
Gender
The association with female gender was examined in 11 studies. Females had a higher risk of having KOA and hand OA, while males were associated with spine OA (22).
Genetic
Only two studies reported an association between having a family history of OA with OA occurrence. Respondents with positive family history were more likely to develop KOA (16).
Modifiable risk factors
Pathophysiological factors
Hypertension
A positive association between hypertension and OA was found in two studies (16, 29). Presence of hypertension was significantly associated with both RKOA and SKOA (29).
Diabetes
The association between diabetes and OA was reported as discovered in two studies (12, 16). The participants with diabetic patients had 2.1 times the odds of developing KOA compared with participants without diabetes (16).
Osteoporosis
Only one study reported on osteoporosis; nonetheless, it failed to demonstrate any significant association between osteoporosis and OA (13).
Presence of KOA
KOA is a significant risk factor for shoulder OA. Prevalence of shoulder OA was higher in participants with KOA (33).
Higher bone mineral density (BMD)
High BMD was significantly associated with an increased risk for RKOA. 0.1g/cm2 increment in BMD raised the risk of KOA by 53% (35).
Lifestyle factors
Obesity
A majority of the studies in this review reported the association between obesity and OA (16 studies). Obesity or high Body Mass Index (BMI) was found to be associated with KOA (20, 22, 23, 36).
Smoking
Smoking habits might be a risk factor for KOA for rural dwellers compared to urban residents (20).
Repetitive use of joints
Repetitive use of joints at work was associated with increased risk of OA (12, 19, 29, 37).
Environmental factors
Poor home ventilation and heating
Only one study discovered an association between home ventilation and heating with OA. Subjects who had lived in well ventilated homes had lower OA than those living under poorly ventilated conditions. Also, subjects who lacked heaters in their homes had a higher prevalence of OA than did others (12).
Area residence
Three studies reported on the association between area residence and OA (26, 36,38). Residents who lived in rural areas or mountainous areas were more likely to develop KOA compared to residents who lived in urban areas (26, 38).
Socioeconomic factors
Lower education
Low educational level indicates low grade occupation. Subjects with a low level of education were more likely to develop OA (12).
Separation, divorce or death
Those who were separated, divorced or widowed were more likely to have OA (12).
Primary prevention of Osteoarthritis
There is not yet a cure for OA, but it has become clear that the management of risk and predisposing factors may slow the disease progression (39). OA management consists of multidisciplinary strategies with the aim to alleviate symptoms and enhance joint functions. The management can be classified into pharmacological and non-pharmacological interventions. In this review, only one study reported on primary prevention of OA (40).
Pharmacological treatment comprises of non-steroidal anti-inflammatory drugs (NSAIDs), analgesics and their combinations which act as first line approach. The majority of general practitioners (GPs) used NSAIDs (61%), followed by analgesics (35%) and a few GPs combined both agents (4%). Non-pharmacological management was under-utilised by most GPs as only 27% advised on exercise, 33% would advise on weight reduction, while seeking for physiotherapist was the least preferred. Other than that, complementary medicines were also used for treatment such as glucosamine, chondroitin, cod liver oil and evening primrose oil (40)
Discussion
OA is the most prevalent form of rheumatic disease and the major cause of disability in Asian countries. In this review, most of the burdens of disability were attributable to the involvement of the knees. Prevalence of OA in the Asian region has kept on increasing due to the ageing population and the rising prevalence of obesity (25, 42).
OA is strongly associated with ageing and the Asian region is aging rapidly. In this review, most of the studies found that the subjects who were aged 50 years and above were more vulnerable to be affected with OA compared to the subjects below 50 years of age (13, 18, 21). A number of factors influence the aging alteration in joint tissues which can lead to OA development. These factors included the development of the senescent secretory phenotype and aging alteration in the matrix due to cell senescence which result in synthesis of advanced glycation end-products that impact the mechanical properties of joint tissues (34).
Majority of the studies in this review reported that being a female and having a high body mass index were significantly associated with knee OA (14, 19, 31) These findings were supported by Nishimura et al. who reported that not only were women more likely to have OA than men, they also have more severe OA (30). The significant prevalence of OA in women around the time of menopause has led to multiple investigations of the hormonal effect on the pathophysiology of OA. However, the results on the effect of estrogen therapy from these investigations have been conflicting as estrogen use is linked to a healthy lifestyle and osteoporosis, which can lower the risk of osteoarthritis (39). Other than that, Zhang et al. reported that having a high body mass index or obesity may cause knee or hip OA. This is because knee and hip joints that withstand long term burden will tear the synovial joint which subsequently lead to ligamentous and other structural support failure (15).
Repetitive use of joints at work is associated with increased risk of OA in almost all of the Asian region(3, 13, 30, 35). According to a research on Osteoarthritis-Osteoporosis Against Disability (ROAD) which was conducted in Japan, occupations involving squatting or kneeling for more than 2 hours per day were associated with high risk of moderate to severe radiographic knee OA. Besides that, the ROAD study also reported that Japanese people aged 60 years and above with an occupation involving climbing for more than 1 hour a day, standing more than 2 hours a day, lifting weights of 10 kg or more at least once a week and walking more than 3 km a day increased risk of radiographic knee OA(35).
High prevalence of OA highlighted the importance of primary prevention. Primary prevention involves pharmacological and non-pharmacological treatments (43). According to Zhang et al. it is important for education programmes to be specific and depend on individual needs, goals and functional capabilities. Patients with OA who have an understanding of the disease tend to cope better and reported less pain. Lifestyle modifications including dietary weight loss and physical active have shown to improve health-related quality of life among OA patients. According to the Framingham Heart Study, the women who had lost 5 kg their weight had lower the risk of symptomatic knee OA development by 50%. This is supported by the same study which reported that weight loss intervention can lower the risk of radiographic knee OA development. This intervention is also shown to be effective among knee OA by minimizing the pain and disability. Another study evaluated the effect of exercise on knee and hip OA and demonstrated an improvement in pain and function (25, 33, 42, 44).
Last but not least, the shortcoming of this scoping review is there was scarce study conducted in Asian countries on the prevalence rates, risk factors and OA primary prevention. Therefore, it is necessary that future collaborative researchers given attention to the overall prevalence rates and guidelines of primary prevention by focusing on lifestyle modification among Asian populations.
Conclusion
High prevalence of knee pain or symptomatic knee OA was observed among Asian elderly in rural and urban areas. Similar findings were also found in other regions worldwide. This issue should be given concern due to current rapid aging and raising obesity cases in most Asian countries. Besides that, simple approach or workplace practices to minimize exposure to continuous heavy manual occupational activities or long term kneeling or squatting should be developed in order to reduce the prevalence of chronic knee pain and disability among Asian population.
Conflict of interest
The author(s) declare(s) no potential conflicts of interests.
Acknowledgements
We would like to express our gratitude to those who have helped in the writing of this article.
Authors' Contribution
Nur Aimi Asyrani Z. and Sakinah H. conceived of the presented idea. Nur Aimi Asyrani Z. screened and collected the data. Sakinah H. supervised the review. Nur Aimi Asyrani Z. wrote the manuscript with support from Ying Qian O., Sakinah H. Noor Aini M.Y. and Nurulhuda M.H. provided critical feedback, shaped the review and provided technical assistance. All authors discussed the results and commented on the manuscript.
References
1. Mobasheri A, Batt M. An update on the pathophysiology of osteoarthritis. Annals of Physcal and Rehabiltation Medicine. 2016; 59(5–6): 333–9.
2. Li Y, Wei X, Zhou J, Wei L. The age-related changes in cartilage and osteoarthritis. BioMed Research International. 2013; 2013: 1-12.
3. Cross M, Smith E, Hoy D, Nolte S, Ackerman I, Fransen M, et al. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Annals of the Rheumatic Diseases. 2014; 73(7) :1323–30.
4. Wittenauer R, Smith L, Aden K. Background paper background paper 6.12 osteoarthritis. World Health Organization. 2013;1–31. Available from: http://www.who.int/medicines/areas/priority_medicines/BP6_12Osteo.pdf
5. Palazzo C, Nguyen C, Lefevre-Colau MM, Rannou F, Poiraudeau S. Risk factors and burden of osteoarthritis. Annals of Physical and Rehabilitation Medicine. 2016; 59(3): 134–8.
6. Bureau USC. An aging world : 2008. Aging. 2009. 7. Johnson VL, Hunter DJ. The epidemiology of osteoarthritis. Best Practice & Research Clinical Rheumatology. 2014; 28(1): 5–15.
8. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology. 2005; 8(1): 19–32.
9. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Medicine. 2009; 6(7):1-6.
10. Jahan I, Sima SH, Khalil M, Sohel MD, Kawsar MH. Survey on prevalence, risk factors and treatment pattern of osteoarthritis in Bangladesh: retrospective study. Rheumatology: Current Research. 2017; 7(4): 1-6.
11. Kolahi S, Khabbazi A, Malek Mahdavi A, Ghasembaglou A, Ghasembaglou A, Aminisani N, et al. Prevalence of musculoskeletal disorders in Azar cohort population in Northwest of Iran. Rheumatology International. 2017; 37(4): 495–502.
12. Zhang JF, Song LH, Wei JN, Zhang AL, Dong HY, Wen HY, et al. Prevalence of and risk factors for the occurrence of symptomatic osteoarthritis in rural regions of Shanxi Province, China. International Journal of Rheumatic Diseases. 2016; 19(8): 781–9.
13. Lee KM, Chung CY, Sung KH, Lee SY, Won SH, Kim TG, et al. Risk factors for osteoarthritis and contributing factors to current arthritic pain in south Korean older adults. Yonsei Medical Journal. 2015; 56(1): 124–31.
14. Davatchi F, Sandoughi M, Moghimi N, Jamshidi AR, Tehrani Banihashemi A, Zakeri Z, et al. Epidemiology of rheumatic diseases in Iran; Adjusted analysis of 4 copcord studies. International Journal of Rheumatic Diseases. 2016; 19(11): 1056-62.
15. Tehrani-Banihashemi A, Davatchi F, Jamshidi AR, Faezi T, Paragomi P, Barghamdi M. Prevalence of osteoarthritis in rural areas of Iran: a WHO-ILAR COPCORD study. International Journal of Rheumatic Diseases. 2014; 17(4): 384–8.
16. Venkatachalam J, Natesan M, Eswaran M, Johnson AKS, Bharath V, Singh Z. Prevalence of osteoarthritis of knee joint among adult population in a rural area of Kanchipuram District, Tamil Nadu. Indian Journal of Public Health. 2017; 62(2): 117–22.
17. Lian W, Liu H, Song Q, Liu YQ, Sun LY, Deng Q, et al. Prevalence of hand osteoarthritis and knee osteoarthritis in Kashin-Beck disease endemic areas and non Kashin-Beck disease endemic areas: A status survey. PLoS One. 2018; 13(1): 1-15.
18. Pal CP, Singh P, Chaturvedi S, Pruthi K, Vij A. Epidemiology of knee osteoarthritis in India and related factors. Indian Journal of Orthopaedics. 2016; 50(5): 518-22.
19. Liu Y, Zhang H, Liang N, Fan W, Li J, Huang Z, et al. Prevalence and associated factors of knee osteoarthritis in a rural Chinese adult population: an epidemiological survey. BMC Public Health. 2016; 16(94): 1–8.
20. Jiang L, Rong J, Zhang Q, Hu F, Zhang S, Li X, et al. Prevalence and associated factors of knee osteoarthritis in a community-based population in Heilongjiang, Northeast China. Rheumatology International. 2012; 32(5): 1189–95.
21. Lee S, Kim S-J. Prevalence of knee osteoarthritis, risk factors, and quality of life: the fifth Korean national health and nutrition examination survey. International Journal of Rheumatic Diseases. 2017; 20(7): 809–17.
22. Cho HJ, Morey V, Kang JY, Kim KW, Kim TK. Prevalence and Risk Factors of Spine, Shoulder, Hand, Hip, and Knee Osteoarthritis in Community-dwelling Koreans Older Than Age 65 Years. Clinical Orthopaedics and Related Research. 2015; 473(10): 3307–14.
23. Ho-Pham LT, Lai TQ, Mai LD, Doan MC, Pham HN, Nguyen TV. Prevalence of radiographic osteoarthritis of the knee and its relationship to self-reported pain. PLoS One. 2014; 9(4): 1–7.
24. Nishimura A, Hasegawa M, Wakabayashi H, Yoshida K, Kato K, Yamada T, et al. Prevalence and characteristics of unilateral knee osteoarthritis in a community sample of elderly Japanese: do fractures around the knee affect the pathogenesis of unilateral knee osteoarthritis?. Journal of Orthopaedic Science. 2012; 17(5): 556–61.
25. Cho HJ, Chang CB, Kim KW, Park JH, Yoo JH, Koh IJ, et al. Gender and prevalence of knee osteoarthritis types in elderly Koreans. The Journal of Arthroplasty. 2011; 26(7): 994–9.
26. Yoshimura N, Muraki S, Oka H, Mabuchi A, En-Yo Y, Yoshida M, et al. Prevalence of knee osteoarthritis, lumbar spondylosis, and osteoporosis in Japanese men and women: The research on osteoarthritis/osteoporosis against disability study. Journal of Bone and Mineral Metabolism. 2009; 27(5): 620–8.
27. Tang X, Wang S, Zhan S, Niu J, Tao K, Zhang Y, et al. The prevalence of symptomatic knee osteoarthritis in china: results from the china health and retirement longitudinal study. Arthritis & Rheumatology. 2016; 68(3): 648–53.
28. YefiL H, Hepgüler S, Öztürk C, Çapaci K, YesiL M. Prevalence of symptomatic knee, hand and hip osteoarthritis among individuals 40 years or older: a study conducted in izmir city. Acta Orthopaedica er Traumatologica Turcica. 2013; 47(4): 231–5.
29. Kim I, Kim HA, Seo Y Il, Song YW, Jeong JY, Kim DH. The prevalence of knee osteoarthritis in elderly community residents in Korea. Journal of Korean Medical Science. 2010; 25(2): 293–8.
30. Nishimura A, Hasegawa M, Kato K, Yamada T, Uchida A, Sudo A. Risk factors for the incidence and progression of radiographic osteoarthritis of the knee among Japanese. International Orthopaedics. 2011; 35(6): 839–43.
31. Yoo JJ, Kim DH, Kim HA. Risk factors for progression of radiographic knee osteoarthritis in elderly community residents in Korea. BMC Musculoskeletal Disorders. 2018; 19(1): 1–7.
32. Muraki S, Akune T, Oka H, Ishimoto Y, Nagata K, Yoshida M, et al. Incidence and risk factors for radiographic knee osteoarthritis and knee pain in Japanese men and women: a longitudinal population-based cohort study. Arthritis and Rheumatism. 2012; 64(5): 1447–56.
33. Oh JH, Chung SW, Oh CH, Kim SH, Park SJ, Kim KW, et al. The prevalence of shoulder osteoarthritis in the elderly Korean population: Association with risk factors and function. Journal of Shoulder and Elbow Surgery. 2011; 20(5): 756–63.
34. Li Y, Wei X, Zhou J, Wei L. The Age-Related Changes in Cartilage and Osteoarthritis. BioMed Resarch International. 2013; 2013: 1-12.
35. Sudo A, Miyamoto N, Horikawa K, Urawa M, Yamakawa T, Yamada T, et al. Prevalence and risk factors for knee osteoarthritis in elderly Japanese men and women. Journal of Orthopaedic Science. 2008; 13(5): 413–8.
36. El Ayoubi N, Chaaya M, Mahfoud Z, Habib R, Uthman I, Slim Z. Risk factors for incident symptomatic knee osteoarthritis: A population-based case control study in Lebanon. International Journal of Rheumatic Diseases. 2013; 16(2): 211–8.
37. Destianti NA, Fatimah SN, Dewi S. Vitamin C intake and risk factors for knee osteoarthritis. Althea Medical Journal. 2017; 4(2): 173–7.
38. Oka H, Akune T, Muraki S, En-Yo Y, Yoshida M, Saika A, et al. Association of low dietary vitamin K intake with radiographic knee osteoarthritis in the Japanese elderly population: Dietary survey in a population-based cohort of the ROAD study. Journal of Orthopaedic Science. 2009; 14(6): 687–92.
39. Muraki S, Oka H, Akune T, Mabuchi A, En-yo Y, Yoshida M, et al. Prevalence of radiographic knee osteoarthritis and its association with knee pain in the elderly of Japanese population-based cohorts: The ROAD study. Osteoarthritis and Cartilage. 2009; 17(9): 1137–43.
40. Anandacoomarasamy A, March L. Current evidence for osteoarthritis treatments. Therapeutic Advances Musculoskeletal Disease. 2010; 2(1): 17–28. 41. Anwar A, Rashid R, Gupta EDAS. A survey of the primary care management of osteoarthritis in Malaysia : a view from a rheumatologist’s perspective. International Journal of Rheumatic Diseases. 2008; 11(3): 246–50.
42. Kang X, Fransen M, Zhang Y, Li H, Ke Y, Lu M, et al. The high prevalence of knee osteoarthritis in a rural Chinese population: the Wuchuan osteoarthritis study. Arthritis and Rheumatism. 2009; 61(5): 641–7. 43. Ratzlaff CR, Liang ML. Prevention of injury related knee osteoarthritis: opportunities for the primary and secondary prevention of knee osteoarthritis. Arthritis Research & Therapy. 2010; 12(215): 1-8.
44. Takeda H, Nakagawa T, Nakamura K, Engebretsen L. Prevention and management of knee osteoarthritis and knee cartilage injury in sports. British Journal of Sports Medicine. 2011; 45(4): 304–9.
Type of Study: Research |
Subject:
General
Received: 2018/11/21 | Accepted: 2019/05/14 | Published: 2019/06/27
Received: 2018/11/21 | Accepted: 2019/05/14 | Published: 2019/06/27
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
