




BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://ehj.ssu.ac.ir/article-1-179-en.html



Uchendu Jude Obiora *1
1. Department of Histopathology, Morbid Anatomy, Delta State University, Abraka, Delta State, Nigeria
Article history
Received 25 Oct 2019
Accepted 19 Feb 2020
A B S T R A C T
Introduction: The elderly represent a significant proportion of the populace and their mortality index is of public health significance. With dearth of vital registration, in-hospital based studies remains a desirable alternative. This study hopes to determine the epidemiologic pattern of elderly mortality with respect to sex, age, date and cause of death.
Methods: This is descriptive retrospective study of elderly deaths among hospitalized patients in a Nigerian Tertiary Care Center. The age, sex, date and causes of death were analyzed using SPSS 21 and results summarized in tables and figures.
Results: Elderly death constitute 24.7% of all hospital deaths with a crude mortality of 25.3%. Males constitute majority of the cases and 81.6% of the deaths occur within the 7th and 8th decades. Non-communicable diseases, communicable diseases and injuries constitute 80%, 12.5% and 7.6% of the cases respectively. Major specific causes of death include cerebrovascular accident, chronic kidney disease, chronic liver disease, sepsis, diabetes mellitus, road traffic accident, prostate and colorectal cancers accounting for 28.8%, 8.7%, 5.7%, 5.3%, 4.9%, 3.8%, 3.4% and 3.0% of all cases respectively.
Conclusion: Mortality rate among in-hospital elderly patients are relatively high. More male are affected than females with causes attributed, in descending order to non- communicable, communicable diseases and external injuries. Major specific causes of death include cerebrovascular accident, chronic liver disease, chronic kidney disease, diabetes mellitus, cancers, sepsis and road traffic injury. Understanding the disease pattern will go a long way guiding social policy and healthcare interventions on the elderly population.
Keywords: Mortality, Non-communicable, Communicable, Injury, Aging
Physiological changes across all organ system in this age group, characterized by degenerative changes, limited regenerative capacity and altered metabolism predisposes them to certain diseases, especially non-communicable diseases (2). Ageing has also been shown to impose a higher risk and adverse clinical outcome on injuries (3).
Understanding the age-specific causes of death in this part of the world is of fundamental importance in enhancing the health outcome and improving longevity. With the inherent unavailability of population-based statistics, hospital based data remaining the best alternative source of data in such countries. This is the first of such study in this region that examines causes of in-hospital death among the elderly patients. Findings in this study will provide a foundation for the needed intervention and policy reforms towards healthy ageing.
Methods
Research design
Delta State is an oil-rich State, located in the South-Sothern part of Nigeria. It has many hospitals at different levels of care. Located within it are two tertiary healthcare centers, one of which is funded by the State (Delta State University Teaching Hospital DELSUTH). This hospital currently has 187-bed capacity but there is an on-going expansion of the facility to accommodate more patients. It serves as the apex hospital of the state and the major referral center to other hospitals operating at lower level within and around the state. The study is a descriptive, retrospective study of elderly patients that died while on admission in the hospital.
Subject selection
The study includes all elderly patients admitted but died within the hospital from 1st January 2016 to 31st December, 2018. Patients above the age of 60 years were considered for this study.
Data collection
The information for this study was retrieved from the record of the Department of Health Information Management of the Hospital. Cases with incomplete information were excluded from the study. Information such age, sex, primary cause of death and the month of death were extracted from the mortality records of the records department of the institution. The causes of death were reclassified according to the International Classification of Diseases (10th revised edition).
Data analysis
These data were analyzed using the SPSS, version 21. The results are summarized in tables and figures.
Ethical considerations
Ethical approval was granted by DELSUTH prior to the commencement of the study (Reference number: DELSUTH/HREC/2019/021/0317).
Results
Two hundred and sixty four deaths were encountered during the 3-year study period, accounting for 24.7% of all hospital deaths, a mean monthly mortality of 7.3 deaths and a crude mortality rate of 25.3%.
Table 1 shows the yearly distribution of in-hospital mortality according to their various age groups. The percentage of deaths in the 6th, 7th, 8th, 9th and 10th decades are 50.2%, 31.4%, 15.2%, 2.3% and 0.4% respectively. The number of deaths recorded in 2016, 2017 and 2018 are 58(22.0%), 102(38.6%) and 104 (39.4%) respectively.
The detail of sex-wise mortality trend from 2016-2018 is shown in figure 1, with an overall male to female ratio of 1.5:1, and a male to female ratio of 1.6:1,1.6:1, and 1.4:1 in 2016, 2017 and 2018 respectively.
The detail of the annual distribution of mortality according to their classes is shown in table 2. Non communicable diseases (NCD), communicable diseases (CD) and external injuries accounted for 211 (80.0%), 33 (12.5%) and 20 (7.6%) of the cases respectively.
The details of the sex distribution of disease mortality are shown in table 3. The male: female ratios for NCD, CD and injuries are 1.3:1, 2:1, and 4:1 respectively.
Thirty-four cancer deaths were encountered in this study. The male to female ratio of cancer mortality is 1.8:1. Prostate, colorectal and hematological malignancies accounted for 9(40.9%), 5(22.7%) and 2(9.0%) respectively of the cancer mortality among males. Ovarian cancer, colorectal cancer and cervical cancer accounted for 4 (33.3%), 3 (25.0%) and 2 (16.7%) respectively of cancer deaths among females. The detail is depicted in table 4.
The details of the frequency of the specific diseases mortality is shown in table 5.
Table 1. Yearly distribution of cases according to various age groups
| Age groups | Yearly distribution of death | Total | ||
| 2016 | 2017 | 2018 | ||
| 61-70 | 30 (51.7%) | 52 (51.0%) | 52 (50.0%) | 134 (50.2%) |
| 71-80 | 18 (31.0%) | 32 (31.4%) | 33 (31.7%) | 83 (31.4%) |
| 81-90 | 8 (13.8%) | 17 (16.7%) | 15 (14.4%) | 40 (15.2%) |
| 91-100 | 1 (1.7%) | 1 (1.0%) | 4 (3.8%) | 6 (2.3%) |
| 101-110 | 1 (1.7%) | 1 (0.4%) | ||
| Total | 58 (100.0) | 102 (100.0) | 104 (100.0) | 264 (100.0) |
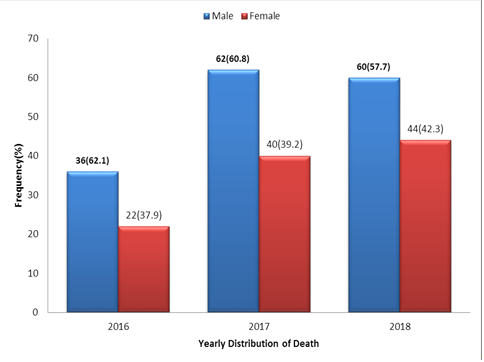
Figure 1. Sex-wise distribution of cases
Table 2. Year-wise distribution of disease and injury mortality 2016-2018
| Cause of death | 2016 (%) | 2017 (%) | 2018 (%) | Total | |
| Injuries | Rood traffic accident | 4 (100.0) | 4 (50.0) | 2 (25.0) | 6 (30) |
| Fall | 2 (25.0) | 2 (25.0) | 4 (20) | ||
| Burns | 2 (25.0) | 2 (10) | |||
| Blunt injury | 2 (25%) | 2 (10) | |||
| Gun injury | 1 (12.5) | 1 (5) | |||
| Suicide (organophosphate) | 1 (12.5) | 1 (5) | |||
| Total | 4 (100.0) | 8 (100.0) | 8 (100.0) | 20 (100) | |
| Communicable infections disease |
CNS infections | 4 (33.3) | 1 (11.1) | 2 (16.72) | 7 (21.2) |
| Urinary tract infection | 1 (8.3) | 1 (3.0) | |||
| Sepsis | 5 (41.7) | 3 (33.3) | 6 (50.0) | 14 (42.4) | |
| Infectious respiratory disease | 2 (16.7) | 3 (33.3) | 3 (25.0) | 8 (24.2%) | |
| Sexual transmitted infection | 2 (22.2) | 1 (8.3) | 3 (9.0) | ||
| Total | 12 (100.0) | 9 (100.0) | 12 (100.0) | 33 (100) | |
| Non Communicable disease | Cerebrovascular | 15 (35.7) | 32 (37.6) | 29 (34.5) | 76 (36.1) |
| Cardiovascular | 3 (7.1) | 7 (8.2) | 6 (7.1) | 16 (7.6) | |
| Endocrine/metabolic disease | 4 (9.5) | 2 (2.4) | 8 (9.5) | 14 (6.6) | |
| Cancer | 3 (7.1) | 19 (22.4) | 12 (14.3) | 34 (16.1) | |
| CNS disease | 1 (2.4) | 2 (2.4) | 3 (1.4) | ||
| Gastrointestinal disease | 3 (7.1) | 7 (8.2) | 6 (7.1) | 16 (7.6 | |
| Genitourinary disease | 2 (4.8) | 7 (8.2) | 6 (7.1) | 15 (7.1) | |
| Genitourinary | 7 (16.7) | 6 (7.1) | 11 (13.1) | 24 (11.4) | |
| Hematological disease | 1 (2.4) | 2 (2.4) | 3 (1.4) | ||
| Respiratory disease | 3 (7.1) | 3 (2.4) | 4 (2.4) | 10 (4.7) | |
| Total | 42 (100.0) | 85 (100.0) | 84 (100.0) | 211 (100) | |
Table 3. Sex distribution of disease mortality
| Disease/Injury entity | Sex | Total(%) | ||
| Male (%) | Female (%) | |||
| Communicable disease |
CNS infection | 5 (22.7) | 2 (18.2) | 7 (21.2) |
| Infectious respiratory disease | 6 (27.3) | 2 (18.2) | 8 (24.2) | |
| Urinary tract infection | 1 (9.1) | 1 (3.0) | ||
| Sepsis | 11 (50.0) | 3 (27.3) | 14 (42.4) | |
| Sexually transmitted infection (AIDS) | 3 (27.3) | 3 (9.1) | ||
| Total | 22 (100.0) | 11 (100.0) | 33 (100) | |
| Non Communicable disease | Cerebrovascular disease | 33 (27.5) | 43 (47.3) | 76 (36.0) |
| CNS disease | 3 (2.5) | 3 (1.4) | ||
| Respiratory disease | 9 (7.5) | 1 (1.1) | 7 (3.3) | |
| Cardiovascular disease | 8 (6.7) | 8 (8.8) | 16 (7.6) | |
| Metabolic disorder | 8 (6.7) | 6 (6.6) | 14 (6.6) | |
| Hematological disease | 2 (1.7) | 1 (1.1) | 3 (1.4) | |
| Genitourinary disease | 19 (15.8) | 5 (5.5) | 24 (11.4) | |
| Gastrointestinal disease | 9 (7.5) | 7 (7.7) | 16 (7.6) | |
| Hepatobiliary disease | 7 (5.8) | 8 (8.8) | 15 (7.1) | |
| Cancers | 22 (18.3) | 12 (13.2) | 34 (16.1) | |
| Total | 120 (100.0) | 91 (100.0) | 211 (100) | |
| Injury | Rood traffic accident | 9 (56.3) | 1 (25.0) | 10 (50.0) |
| Fall | 3 (18.8) | 1 (25.0) | 4 (20.0) | |
| Blunt injury/Physical assault | 1 (6.3) | 1 (25.0) | 2 (10.0) | |
| Burns | 1 (6.3) | 1 (25.0) | 2 (5.0) | |
| Suicide (organophosphate) | 1 (6.3) | 1 (5.0) | ||
| Gun shot | 1 (6.3) | 1 (5.0) | ||
| Total | 16 (100.0) | 4 (100.0) | 20 (100) | |
| Organ/region | Male | Female |
| Pancreatic cancer | 1 (4.5) | |
| Prostate cancer | 9 (40.9) | |
| Colorectal cancer | 5 (22.7) | 3 (25.0) |
| Gastric cancer | 1 (4.5) | |
| Head and neck tumour | 1 (4.5) | |
| Hematological cancer | 2 (9.0) | |
| Liver cancer | 1 (4.5) | |
| Soft tissue cancer | 1 (4.5) | 1 (8.3) |
| Breast cancer | 1 (8.3) | |
| Cervical cancer | 2 (16.7) | |
| CNS tumour | 1 (4.5) | 1 (8.3) |
| Ovarian cancer | 4 (33.3) | |
| Total | 22 (100.0) | 12 (100.0) |
Granted that the study is a hospital-based study, its finding is very significant as it depicts elderly disease mortality trend in the region of the country served by the hospital. Besides, non-consistent vital registration and rarity of census is an obvious challenge limiting data availability in most developing countries (4).
In this study, we observed a total of 264 deaths out of 1070 deaths, representing 24.7% of all deaths in the hospital and a crude mortality rate of 25.3%. Our report is intermediate between the values observed by Sanya et al. (22.4%) in Middle belt (5) and Arodiwe et al. (31.2%) in South Eastern Nigeria (6), but higher than values observed by Lamont et al. (20%) in USA (7), Shoko et al (17.7%) in Japan (8) and Silva et al. (16.4%) in Brazil (9). The discrepancy in crude mortality rate between high and low income countries may be attributed to limited healthcare resources as well as lack of experts in geriatric medicine in the later.
We observed an increase in number of mortality across the years. We think that this may be attributed to the ongoing expansion of the hospital facility and establishment of new departments, resulting in increase in number of referrals from peripheral primary and secondary healthcare centers.
| Disease | Frequency | Percentage |
| Cerebrovascular accident | 76 | 28.8 |
| Chronic kidney disease | 23 | 8.7 |
| Chronic liver disease | 15 | 5.7 |
| Sepsis | 14 | 5.3 |
| Diabetes mellitus | 13 | 4.9 |
| Road traffic accident | 10 | 3.8 |
| Prostate cancer | 9 | 3.4 |
| Colectal cancer | 8 | 3.0 |
| Congestive cardiac failure | 8 | 3.0 |
| Peptic ulcer disease | 8 | 3.0 |
| Pneumonia | 6 | 2.3 |
| Meningitis/Encephalitis | 6 | 2,3 |
| Severe hypertension | 5 | 1.9 |
| Ovarian cancer | 4 | 1.5 |
| Chronic obstructive Airway disease | 4 | 1.5 |
| Intestinal obstruction | 4 | 1.5 |
| Fall from height | 4 | 1.5 |
| Retroviral disease | 3 | 1.1 |
| Cervical cancer | 2 | 0.8 |
| Sarcoma | 2 | 0.8 |
| Severe anaemia | 2 | 0.8 |
| Pneumonia | 2 | 0.8 |
| Acute asthmatic attack | 2 | 0.8 |
| Assault | 2 | 0.8 |
| Burns | 2 | 0.8 |
| Others | 30 | 11.4 |
| Total | 264 | 100 |
The age distribution of the patients shows a mean age of 72 (6). Age range of 60-103 years, with 81.6% of the deaths within the 7th and 8th decade. This result closely tallies with those observed in the middle belt (68 years) (5) and south eastern Nigeria (69.9%) (6). This invariably depicts the population curve of the elderly populace and may be relevant in designing a mortality and population predicting model for old people in the backdrop of absent vital registration system (4) The dearth of government and institutional involvement in supporting the elderly population, and dependence on family members for their healthcare funding is the trend in most developing countries (10). The high cost of caring for the health need of the elderly populace may impact on their access to healthcare especially where the family members are not economically fit. In contrast, most developed countries have better welfare package for the elderly, better standard of living, and more sophisticated medical care all of which contribute to increasing longevity (11).
This study showed that male mortality is higher than that of the female among the elderly with a male to female ratio of 1.5:1. This is comparable with a ratio of 1.4:1 and 1.7:1 observed in Middle belt (5), and south eastern Nigeria (6) respectively. At global level, adult mortality has been shown to be naturally higher among the male gender (12). The relatively higher life expectancy of adult females is attributed to inherent biological advantage, less involvement in risky behaviors or unhealthy lifestyles and lastly because they seem to benefit more from health policies (12).
We observed more death from NCDs than those from communicable diseases or external injuries, which is in agreement with studies in other parts of the country (5, 6, 13). This is also in line with the report that about 80% of NCDs occur in low and middle income countries and that 75% of global NCD-deaths occur among 60+ year’s individuals (14). The high rate of NCD related mortality are rooted in unhealthy life-style changes and habit much earlier in the life cycle such as alcohol consumption, smoking, unhealthy eating habits, insufficient physical activity or even occupational risk factor exposures, and poor management of hypertension. Modification of exposure to these risk factors at younger age will invariably translate to headier elders in the society (15). In this study the most common causes of NCD mortality are cerebrovascular events, chronic kidney disease, chronic liver disease and diabetes mellitus. Leading causes in injury related mortality are rood traffic accident and fall; while leading causes of infection mortality are sepsis, respiratory tract and central nervous system infections.
The single most common cause of death in this study is cerebrovascular accident (CVA) which accounted for 28.8% of all deaths. CVA has earlier been reported as the most common cause of elderly mortality by Uchendu et al. in South South, Sanya in Middle Belt and Arodiwe in South Eastern Nigeria representing 25.1%, 19.8% and 19.3% of deaths respectively (5, 6, 13). In a country with dearth of imaging equipment or specialists in geriatric medicine, under-diagnosis is likely, implying that proportion of CVAs quoted in these studies are likely to be an underrepresentation. Across the globe, stroke is the second single most common cause of death (after ischemic heart disease), accounting for 11.8% of all deaths (16). The role of hypertension and lifestyle cannot be overemphasized (15).
Cancer death accounted for 12.9% of deaths in this study, with the duo of prostatic and colorectal cancer being the most common causes in males while colorectal and ovarian cancer are the most common causes among females. Observation in this study is lower than the incidence observed by Uchendu and Forae in South Southern Nigeria (15.2%) (13), but higher than value reported in Middle belt (8.4%) (5) and South-Eastern Nigeria(4.6%) (6). From global perspective, studies has shown that 60% of diagnosed cancer cases and 70% of cancer mortality occur among the elderly populace (17). It is my opinion that cancer-related mortality will continue to rise with increasing population of the elderly, limited availability of cancer screening techniques, late diagnosis and unavailability of specialized cancer treatment facilities; except if desirable steps are taken to reverse this trend.
Infections are relatively common in this study, accounting for 12.5% of the cases. Sepsis, central nervous system and respiratory infections accounted for most cases. Age-related decline in immune response, co-morbidities, functional impairment and increasing duration and number of hospital admission that characterize the elderly patients are the likely explanations.
Fatal external injuries are relatively common accounting for 7.5% of the cases which is higher than the value of 4.4% reported by Sanya et al. in the Middle belt zone of the country (5). Fatal injuries mortality has earlier been shown to be relatively high among the elderly populace in this study using autopsy data, the differences arising from difference in inclusion criteria used for both studies (18). In a study in South Eastern Nigeria, Onyemaechi reported that rood traffic accident is the leading cause of injury-related hospital mortality (19). Fall, the second cause of fatal injury in this study, is also relatively common in this age group among European countries and US (20, 21). Only one case of suicide which was executed by ingesting organ phosphorus organophosphate poison was identified in this study, supporting the earlier report of rarity of suicide in this region (22).
Conclusion
Mortality among in-hospital elderly patients are relatively high. More male are affected than females And causes are attributed, in descending order to non-communicable, communicable diseases and external injuries. Major specific causes of death include CVA, chronic liver disease, chronic kidney disease, Diabetes mellitus, cancers, sepsis and RTA. Understand the disease pattern will go a long way guiding social policy and healthcare interventions on the elderly population.
Study limitations
Documentation of mortality by Hospital Staff is poor, leading to loss of data. Filing of patients’ case notes is a serious problem. Also since this study is based on patients that utilize the hospital service, it may not be an exact representation of the true population statistics.
Conflict of interest
The author has no conflict of interest to declare.
Acknowledgments
The author wish to thank staff and management of Delta State University Teaching Hospital, Nigeria for their support in the conduct of this research.
Authors’ contributions
The entire reseach work from the conception to the end was executed by the Uchendu Jude Obiora.
Reference
-
Akanji BO, Ogunniyi A, Bayewu O. Healthcare for elderly persons, a country profile: Nigeria. Journal of the American Geriatrics Society. 2002; 50(7): 1289-92.
-
Boss GR, Seegmiller JE. Age-related physiological changes and their clinical significance. The Western Journal of Medicine. 1981; 135(6): 434–40.
-
Poulose N, Raju R. Aging and injury: alterations in cellular energetics and organ function. Aging and Disease. 2014; 5(2): 101-8.
-
Mathers CD, Ma Fat D, Inoue M, Rao C, Lopez AD. Counting the dead and what they died from: an assessment of the global status of cause of death data. Bulletin of the World Health Organization. 2005; 83: 171–7.
-
Sanya EO, Abiodun AA, Kolo P, Olanrewaju TO, Adekeye K. Profile and causes of mortality among elderly patients seen in a tertiary care hospital in Nigeria. Annals of African Medicine. 2011; 10(4): 278-83.
-
Arodiwe EB, Nwokediuko SC, Ike SO, Ulasi II, Ijoma CK, Chiwuba KI. Medical causes of death among the elderly in a tertiary hospital internal medicine ward, South East Nigeria. The West Indian Medical Journal. 2017; 66(1): 50-5.
7.Lamont CT, Sampson S, Matthias R, Kane R. The outcome of hospitalization for acute illness in the elderly. Journal of the American Geriatrics Society. 1983; 31(5): 282-8
-
Shoko T, Shiraishi A, Kaji M, Otomo Y. Effects of pre-existing medical conditions on in-hospital mortality: Analysis of 20,257 trauma patients in Japan. Journal of the American College of Surgeons. 2010; 211(3): 338-46.
-
Avelino-Silva TJ, Szlejf C, Farfel J, Curiati JA, Jacob-Filho W. Predictors of in-hospital mortality among older patients. Clinics (Sao Paulo). 2009; 64(7): 613-8.
-
Bendavid E, Seligman B, Kubo J. (2011) Comparative analysis of old-age mortality estimations in Africa. PLoS ONE. 2011; 6(10): e26607.
-
Christensen K, Doblhammer G, Rau R, Vaupel JW. Ageing population: the challenges ahead. Lancet. 2009; 374(9696): 1196-208.
-
United Nations. World Mortality Report 2015 –Highlights. New York: Department of Economic and Social Affairs, 2017.
-
Uchendu OJ, Forae DJ. Diseases mortality patterns in elderly patients: A Nigerian teaching hospital experience in Irrua, Nigeria. Nigerian Medical Journal. 2013; 54 (4): 250-3.
-
World Health Organization. Global status report on non-communicable diseases 2010 [Internet]. 2011. Available from: https://apps.who.int/iris/bitstream/handle/10665/44579/9789240686458_eng.pdf?sequence=1
-
World Health Organization. Global status report on non-communicable diseases 2014: attaining the nine global non-communicable diseases targets; a shared responsibility [Internet]. 2014. Available from: https://apps.who.int/iris/bitstream/handle/10665/148114/9789241564854_eng.pdf.
-
Feigin, VL, Norrving B, Mensah GA. Global burden of stroke. Circulation Research. 2017; 120(3): 439-449.
-
Alan Ö, Gürsel Ö, Ünsal M, Altın S, Kılçıksız S. Oncologic Approach in Geriatric Patients. Okmeydanı Tıp Dergisi. 2013; 29(2): 94–8.
-
Ijomone EA, Uchendu OJ, Nwachokor FN. A study of elderly deaths in Medicolegal autopsies performed in Warri, Nigeria. Journal of Dental and Medical Sciences. 2017; 16 (6): 61-4.
-
Onyemaechi NO, Nwankwo OE, Ezeadawi RA. Epidemiology of injuries seen in a Nigerian tertiary hospital. Nigerian Journal of Clinical Practice. 2018; 21(6): 752-7.
-
Tinetti ME. Preventing falls in elderly persons. The New England Journal of Medicine. 2003; 348: 42-9.
-
Stevens JA, Rudd Ra. Circumstance and contributing causes of fall deaths among persons aged 65 and older: United States, 2010. Journal of the American Geriatrics Society. 2014; 62(3): 470-5.
-
Uchendu OJ, Ijomone EA, Nwachokor NF. Suicide in Warri, Delta State, Nigeria: An autopsy study. Annals of tropical Pathology. 2019; 10; 16-9.
Received: 2019/10/25 | Accepted: 2020/02/19 | Published: 2020/06/27
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
