

Volume 12, Issue 1 (June 2026)
Elderly Health Journal 2026, 12(1): 8-16 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Dehghan Niri E, Haj Lotfalian M, Zare Bidoki F. The Effect of Mind-Body Relaxation Exercises on Gait Smoothness and Gait Profile in Elderly Women. Elderly Health Journal 2026; 12 (1) :8-16
URL: http://ehj.ssu.ac.ir/article-1-370-en.html
URL: http://ehj.ssu.ac.ir/article-1-370-en.html



Department of Physical Education and Sport Sciences, Faculty of Psychology and Educational Sciences, Yazd University; Yazd: Iran , m.hajlotfalian@yazd.ac.ir
Full-Text [PDF 508 kb]
(34 Downloads)
| Abstract (HTML) (121 Views)
Full-Text: (16 Views)
The Effect of Mind-Body Relaxation Exercises on Gait Smoothness and Gait Profile in Elderly Women
Elham Dehghan Niri 1, Mostafa Haj Lotfalian 2 * , Fateme Zare Bidoki 3
A B S T R A C T
Introduction
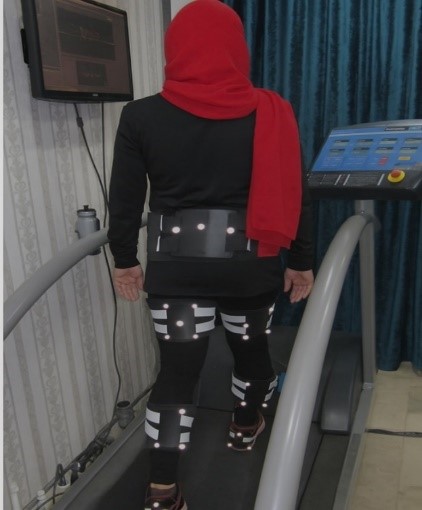
Figure 1. A participant performing the walking task on the treadmill
Table 1. Descriptive characteristics of participants (Mean ± SD)
Table 2. Results of the two-way mixed-design repeated measures ANOVA for movement smoothness and gait profile score
.png)
Figure 2. Movement smoothness values across pre-test and post-test assessments in the experimental and control groups. Bars represent mean values, error bars indicate standard deviation, and scatter points represent individual participant data.
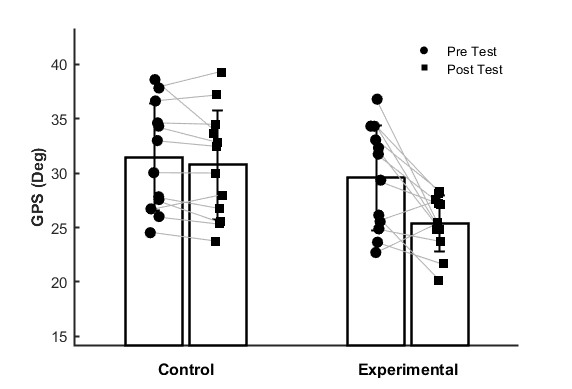
Figure 3. Gait Profile Score across pre-test and post-test assessments in the experimental and control groups. Bars represent mean values, error bars indicate standard deviation, and scatter points represent individual participant data.
Discussion
Elham Dehghan Niri 1, Mostafa Haj Lotfalian 2 *
- Department of Behavioral and Cognitive Sciences in Sport, Faculty of Sports and Health Sciences, University of Tehran, Tehran, Iran
- Department of Physical Education and Sport Sciences, Faculty of Psychology and Educational Sciences, Yazd University; Yazd: Iran
- Department of Sports Injury and Biomechanics, Faculty of Sports and Health Sciences, University of Tehran, Tehran, Iran
Article history
Received 15 Nov 2025
Accepted 10 Jun 2026
Received 15 Nov 2025
Accepted 10 Jun 2026
A B S T R A C T
Introduction: The present study aimed to investigate the effects of mind‑body relaxation exercises on qualitative gait parameters, including movement smoothness and gait profile, in elderly women. This research focuses on how such interventions might enhance gait quality, potentially by strengthening core muscles, improving pelvic stability, and boosting neuromuscular coordination, which could play a vital role in optimizing gait patterns and reducing fall risk among this population.
Methods: In this quasi-experimental study, twenty‑four elderly women aged over 55 years voluntarily participated and were randomly assigned to either an experimental or a control group. The experimental group engaged in a six-week training program consisting of three sessions per week. Gait kinematic data were recorded using a three-dimensional motion capture system at a sampling rate of 120 Hz. The smoothness index was calculated based on the integral of angular jerk, whereas the gait profile score was determined as the mean deviation of joint angles from a normative gait pattern. Data were analyzed using two-way repeated measures ANOVA.
Results: The results demonstrated no significant main effects of group or time, nor a significant group × time interaction, for the movement smoothness index (all p > 0.05). In contrast, for the gait profile score, significant main effects of group (p = 0.041) and time (p = 0.001), as well as a significant group × time interaction effect (p = 0.016), were observed. These findings indicate that the six-week mind–body exercise intervention significantly improved gait movement patterns and reduced gait deviations in elderly women, whereas no significant changes were observed in movement smoothness.
Conclusion: Mind-body relaxation exercises appear to enhance gait patterns and reduce fall risk in elderly women through mechanisms such as core muscle strengthening, pelvic stability improvement, and better neuromuscular coordination. Nevertheless, the lack of significant change in smoothness suggests that assessing the effects of these interventions on fine motor control may require longer training periods and more sensitive measurement tools.
Keywords: Aging, Gait Analysis, Mind-Body Therapies, Gait, Postural Balance
Copyright © 2026 The Author(s). This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/) which permits copy and redistribute the material just in noncommercial usages, provided the original work is properly cite.
Methods: In this quasi-experimental study, twenty‑four elderly women aged over 55 years voluntarily participated and were randomly assigned to either an experimental or a control group. The experimental group engaged in a six-week training program consisting of three sessions per week. Gait kinematic data were recorded using a three-dimensional motion capture system at a sampling rate of 120 Hz. The smoothness index was calculated based on the integral of angular jerk, whereas the gait profile score was determined as the mean deviation of joint angles from a normative gait pattern. Data were analyzed using two-way repeated measures ANOVA.
Results: The results demonstrated no significant main effects of group or time, nor a significant group × time interaction, for the movement smoothness index (all p > 0.05). In contrast, for the gait profile score, significant main effects of group (p = 0.041) and time (p = 0.001), as well as a significant group × time interaction effect (p = 0.016), were observed. These findings indicate that the six-week mind–body exercise intervention significantly improved gait movement patterns and reduced gait deviations in elderly women, whereas no significant changes were observed in movement smoothness.
Conclusion: Mind-body relaxation exercises appear to enhance gait patterns and reduce fall risk in elderly women through mechanisms such as core muscle strengthening, pelvic stability improvement, and better neuromuscular coordination. Nevertheless, the lack of significant change in smoothness suggests that assessing the effects of these interventions on fine motor control may require longer training periods and more sensitive measurement tools.
Keywords: Aging, Gait Analysis, Mind-Body Therapies, Gait, Postural Balance
Copyright © 2026 The Author(s). This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/) which permits copy and redistribute the material just in noncommercial usages, provided the original work is properly cite.
Introduction
Aging, even in the absence of chronic disease, is accompanied by various biological changes that contribute to the reduction of skeletal muscle mass, strength, and function. This can lead to an overall decrease in physiological resilience (the ability to withstand and recover from stressors) and increased vulnerability to catastrophic events (1). The global population aged 80 years and over is projected to triple, rising from 143 million in 2019 to 426 million in 2050 (2). Gait disorder is a common syndrome in old age that can lead to problems such as short step length, increased variability in walking patterns, a high risk of falling, and limitations in daily physical activity among older adults (over 65 years). Approximately 29% of older adults experience at least one fall per year, and nearly 10% of these falls result in serious injuries such as hip fractures (3). Since gait impairment itself, falling, or reduced physical activity are among the most important causes of loss of independence, decreased quality of life, and increased mortality in the elderly (4), implementing preventive measures against gait disorders in this vulnerable group is essential.
Human movement, particularly in the form of walking, is the result of a complex interaction between the nervous, muscular, and skeletal system (5). A detailed analysis of the qualitative characteristics of gait can provide deep insight into the functional status of these systems. One important metric in this context is movement smoothness, which indicates the uniformity, continuity, and efficiency of neuromuscular control during movement execution. High smoothness reflects fluid, coordinated movement without sudden changes in acceleration, whereas reduced smoothness suggests the presence of compensatory movements, fine tremors, and a decline in neural control. From a biomechanical perspective, the smoothness metric is typically measured by analyzing jerk, which is the third derivative of displacement with respect to time (6). A reduction in jerk signifies more optimal and natural movement, characterized by lower energy consumption and reduced neuromuscular stress (7). In the context of gait disorders in older adults, multifaceted biomechanical and neuromuscular changes are revealed. With advancing age, gait typically becomes less efficient, characterized by decreased step length, increased variability, slower speed, and reduced smoothness—often measured by metrics such as harmonic ratios or spectral analysis of acceleration signals. These changes increase the risk of falling by impairing postural stability and adaptive responses to perturbations (8, 9). In this regard, mind-body interventions, including Pilates, are proposed as effective strategies for mitigating these issues. Foundational studies have demonstrated that a 12-week Pilates program significantly improved dynamic balance, muscle strength, and reaction time in women over 65 years of age, and led to a substantial reduction in falls—from an average of 1.87 to 0.37 falls per participant (10).
In general, among older adults, factors such as muscular weakness, diminished proprioceptive input, and limited joint range of motion cause the gait pattern to deviate from its normal state, resulting in significant alterations in the movement profile (9). The combination of the two metrics of smoothness and gait profile provides a comprehensive picture of motor control quality and can serve as a scientific basis for evaluating the effectiveness of exercise interventions (9).
Recent studies have reported that Pilates exercises are suitable for all ages, body types, and physical abilities due to the adaptable nature of their movements (11). In this context, a 2022 randomized controlled trial by Aibar-Almazán et al., demonstrated that 12 weeks of Pilates training led to significant improvements in gait speed (effect size = 0.87) and handgrip strength in sedentary community-dwelling older women (12). Aligned with this study, the results of a comprehensive review and meta-analysis reported small to moderate effects of Pilates on dynamic balance and functional capacity, attributing the benefits to improved neuromuscular coordination, which can positively influence gait patterns (13).
Although the conducted studies generally support the benefits of this type of exercise, numerous inconsistencies and limitations persist in the research. In this regard, one can point to a scarcity of investigations that employ precise biomechanical tools, such as motion capture systems, to quantify changes in gait smoothness through metrics like harmonic ratios. While simple mobility tests (e.g., the 6-minute walk test and the Timed Up and Go test) are practical, they do not allow for a detailed analysis of how specific gait patterns may increase the risk of falling (14). In contrast, gait biomechanics analyzed using 3D motion capture systems can precisely record human movement and quantify fall risk by examining foot kinematics and dynamic balance (15). Another issue is that older women are at a higher risk for hip fractures and are more likely to develop a fear of falling after experiencing a fall (16). Therefore, to prevent falls and improve the quality of life for the elderly, particularly older women, advancing the current understanding of the effects of aging on their dynamic balance capabilities is crucial.
The present study addresses this knowledge gap by investigating Pilates exercises, which are among the most effective mind-body relaxation methods. By strengthening core muscles, increasing flexibility, and improving pelvic stability, these exercises can enhance the gait pattern. Through improved motor control and reduced compensatory movements, such exercises can increase movement smoothness and shift the gait profile closer to the natural pattern.
Therefore, given the importance of maintaining mobility and preventing falls in the elderly population, it is essential to evaluate the effectiveness of mind-body relaxation exercises on movement quality using precise biomechanical metrics. Accordingly, the objective of the present study is to investigate the effect of these exercises on two key metrics—
movement smoothness and gait profile—in elderly women. This will be achieved through a comprehensive analysis of kinematic data to provide a detailed picture of changes in gait quality and improvements in neuromuscular control resulting from these exercises.
Method
Participants
In this study, 24 elderly women over the age of 55 voluntarily participated. The participants were identified through announcements at daily senior centers and women's sports clubs. After screening, participants were deemed eligible if they met the following inclusion criteria: age over 55 years, no history of lower limb injury or surgery in the previous six months, no severe balance or neurological disorders, and a score of "poor" (less than 12) on the Functional Movement Screen. Due to the limited accessibility of eligible elderly participants who met the study criteria, recruitment was restricted to 24 participants. However, considering the repeated-measures design of the study, an acceptable statistical power (0.80) and a moderate expected effect size were taken into account to justify the sample size adequacy. In addition, balanced group allocation was used to improve the sensitivity and stability of the statistical analyses. Following the baseline assessment, participants were randomly assigned into experimental and control groups (n = 12 per group) using computer-generated random allocation software. In addition, the researcher responsible for processing and analyzing the motion capture data was blinded to group allocation in order to minimize potential assessment bias.
Procedure
First, personal information and anthropometric characteristics of the participants were recorded. The study was conducted in Yazd, Iran. All baseline and post-intervention assessments, including gait analysis and kinematic data collection, were performed at the Biomechanics Laboratory of Yazd University.
Participants in the control group were instructed to maintain their usual daily activities throughout the study period and to refrain from participating in any new structured exercise programs or additional sports classes during the intervention period.
Prior to data collection, all participants completed two familiarization sessions with treadmill walking. During these sessions, participants practiced walking on the treadmill until they demonstrated a stable and natural gait pattern without observable signs of discomfort, hesitation, or gait alteration. Preferred walking speed was determined by gradually adjusting treadmill speed based on participant feedback until a comfortable and natural walking pace was achieved. The same preferred speed obtained during the pre-test session was maintained during the post-test assessment to ensure consistency of gait measurements.
For kinematic data collection, a three-dimensional motion capture system (OptiTrack V120 Duo, USA) with an accuracy of less than 0.5 mm, as specified by the manufacturer, and a sampling rate of 120 Hz was used. Reflective markers were applied in clusters on the pelvis, thigh, shank, and foot segments to minimize errors due to skin movement artifact.
After assuming a standard anatomical standing position, participants walked on the Hp Cosmos Mercury treadmill (Germany) at their predetermined preferred speed. Data collection was performed under steady-state conditions for a minimum of 30 seconds to capture at least 10 complete gait cycles. To ensure data reliability and availability, the testing procedure was repeated three times with a one-minute rest interval between trials. (Figure 1)
Human movement, particularly in the form of walking, is the result of a complex interaction between the nervous, muscular, and skeletal system (5). A detailed analysis of the qualitative characteristics of gait can provide deep insight into the functional status of these systems. One important metric in this context is movement smoothness, which indicates the uniformity, continuity, and efficiency of neuromuscular control during movement execution. High smoothness reflects fluid, coordinated movement without sudden changes in acceleration, whereas reduced smoothness suggests the presence of compensatory movements, fine tremors, and a decline in neural control. From a biomechanical perspective, the smoothness metric is typically measured by analyzing jerk, which is the third derivative of displacement with respect to time (6). A reduction in jerk signifies more optimal and natural movement, characterized by lower energy consumption and reduced neuromuscular stress (7). In the context of gait disorders in older adults, multifaceted biomechanical and neuromuscular changes are revealed. With advancing age, gait typically becomes less efficient, characterized by decreased step length, increased variability, slower speed, and reduced smoothness—often measured by metrics such as harmonic ratios or spectral analysis of acceleration signals. These changes increase the risk of falling by impairing postural stability and adaptive responses to perturbations (8, 9). In this regard, mind-body interventions, including Pilates, are proposed as effective strategies for mitigating these issues. Foundational studies have demonstrated that a 12-week Pilates program significantly improved dynamic balance, muscle strength, and reaction time in women over 65 years of age, and led to a substantial reduction in falls—from an average of 1.87 to 0.37 falls per participant (10).
In general, among older adults, factors such as muscular weakness, diminished proprioceptive input, and limited joint range of motion cause the gait pattern to deviate from its normal state, resulting in significant alterations in the movement profile (9). The combination of the two metrics of smoothness and gait profile provides a comprehensive picture of motor control quality and can serve as a scientific basis for evaluating the effectiveness of exercise interventions (9).
Recent studies have reported that Pilates exercises are suitable for all ages, body types, and physical abilities due to the adaptable nature of their movements (11). In this context, a 2022 randomized controlled trial by Aibar-Almazán et al., demonstrated that 12 weeks of Pilates training led to significant improvements in gait speed (effect size = 0.87) and handgrip strength in sedentary community-dwelling older women (12). Aligned with this study, the results of a comprehensive review and meta-analysis reported small to moderate effects of Pilates on dynamic balance and functional capacity, attributing the benefits to improved neuromuscular coordination, which can positively influence gait patterns (13).
Although the conducted studies generally support the benefits of this type of exercise, numerous inconsistencies and limitations persist in the research. In this regard, one can point to a scarcity of investigations that employ precise biomechanical tools, such as motion capture systems, to quantify changes in gait smoothness through metrics like harmonic ratios. While simple mobility tests (e.g., the 6-minute walk test and the Timed Up and Go test) are practical, they do not allow for a detailed analysis of how specific gait patterns may increase the risk of falling (14). In contrast, gait biomechanics analyzed using 3D motion capture systems can precisely record human movement and quantify fall risk by examining foot kinematics and dynamic balance (15). Another issue is that older women are at a higher risk for hip fractures and are more likely to develop a fear of falling after experiencing a fall (16). Therefore, to prevent falls and improve the quality of life for the elderly, particularly older women, advancing the current understanding of the effects of aging on their dynamic balance capabilities is crucial.
The present study addresses this knowledge gap by investigating Pilates exercises, which are among the most effective mind-body relaxation methods. By strengthening core muscles, increasing flexibility, and improving pelvic stability, these exercises can enhance the gait pattern. Through improved motor control and reduced compensatory movements, such exercises can increase movement smoothness and shift the gait profile closer to the natural pattern.
Therefore, given the importance of maintaining mobility and preventing falls in the elderly population, it is essential to evaluate the effectiveness of mind-body relaxation exercises on movement quality using precise biomechanical metrics. Accordingly, the objective of the present study is to investigate the effect of these exercises on two key metrics—
movement smoothness and gait profile—in elderly women. This will be achieved through a comprehensive analysis of kinematic data to provide a detailed picture of changes in gait quality and improvements in neuromuscular control resulting from these exercises.
Method
Participants
In this study, 24 elderly women over the age of 55 voluntarily participated. The participants were identified through announcements at daily senior centers and women's sports clubs. After screening, participants were deemed eligible if they met the following inclusion criteria: age over 55 years, no history of lower limb injury or surgery in the previous six months, no severe balance or neurological disorders, and a score of "poor" (less than 12) on the Functional Movement Screen. Due to the limited accessibility of eligible elderly participants who met the study criteria, recruitment was restricted to 24 participants. However, considering the repeated-measures design of the study, an acceptable statistical power (0.80) and a moderate expected effect size were taken into account to justify the sample size adequacy. In addition, balanced group allocation was used to improve the sensitivity and stability of the statistical analyses. Following the baseline assessment, participants were randomly assigned into experimental and control groups (n = 12 per group) using computer-generated random allocation software. In addition, the researcher responsible for processing and analyzing the motion capture data was blinded to group allocation in order to minimize potential assessment bias.
Procedure
First, personal information and anthropometric characteristics of the participants were recorded. The study was conducted in Yazd, Iran. All baseline and post-intervention assessments, including gait analysis and kinematic data collection, were performed at the Biomechanics Laboratory of Yazd University.
Participants in the control group were instructed to maintain their usual daily activities throughout the study period and to refrain from participating in any new structured exercise programs or additional sports classes during the intervention period.
Prior to data collection, all participants completed two familiarization sessions with treadmill walking. During these sessions, participants practiced walking on the treadmill until they demonstrated a stable and natural gait pattern without observable signs of discomfort, hesitation, or gait alteration. Preferred walking speed was determined by gradually adjusting treadmill speed based on participant feedback until a comfortable and natural walking pace was achieved. The same preferred speed obtained during the pre-test session was maintained during the post-test assessment to ensure consistency of gait measurements.
For kinematic data collection, a three-dimensional motion capture system (OptiTrack V120 Duo, USA) with an accuracy of less than 0.5 mm, as specified by the manufacturer, and a sampling rate of 120 Hz was used. Reflective markers were applied in clusters on the pelvis, thigh, shank, and foot segments to minimize errors due to skin movement artifact.
After assuming a standard anatomical standing position, participants walked on the Hp Cosmos Mercury treadmill (Germany) at their predetermined preferred speed. Data collection was performed under steady-state conditions for a minimum of 30 seconds to capture at least 10 complete gait cycles. To ensure data reliability and availability, the testing procedure was repeated three times with a one-minute rest interval between trials. (Figure 1)
Intervention protocol
The experimental group participated in a six-week mind-body exercise program (three sessions per week, each lasting 60 minutes). Each session consisted of three parts: a warm-up (10 minutes), main exercises (40 minutes) including stretching, strengthening, and trunk control exercises in supine, sitting, and standing positions, and a cool-down (10 minutes) focusing on breathing and muscle relaxation. The intensity of the exercises was progressively increased from simple mat-based movements to combined exercises using an aerobic ball, resistance bands, and light weights.
The six-week intervention period was selected primarily based on participant availability, adherence considerations, and the feasibility of maintaining regular attendance among older adults. Although longer intervention durations have been reported in previous studies, the present protocol was designed to investigate the short-term effects of mind-body exercise on gait-related motor control parameters. Nevertheless, it should be acknowledged that a six-week duration may be insufficient to induce larger adaptations in sensitive movement control variables such as gait smoothness. The control group maintained their usual daily activities throughout the study period and were instructed not to participate in any additional structured exercise programs. After the six-week intervention period, the gait assessment was repeated for both groups following the same protocol used during the pre-test.
Results processing
Following data collection, initial processing was performed in Motive software, and the final analysis was conducted in MATLAB version 2021. The kinematic data were processed using a Gaussian low-pass filter with a cutoff frequency of 6 Hz to reduce signal noise and reconstruct occasional missing marker trajectories. After identifying the different gait phases using the positions of the markers attached to the foot, joint angles were calculated from the marker positions using an inverse kinematics approach. For each participant, a minimum of 10 complete gait cycles were analyzed. To improve measurement consistency, all data collection procedures, marker placements, and motion capture assessments were conducted by the same experienced examiner under identical laboratory conditions. Therefore, formal intra-rater and inter-rater reliability analyses (e.g., ICC) were not separately calculated in the present study.
The movements of the pelvis and hips in the three anatomical planes, along with the movements of the knees and ankles in the sagittal plane, and foot progression, constituted the 15 degrees of freedom that were estimated from the kinematic information. Subsequently, the values for the Smoothness Index and the Gait Profile Score were calculated.
Calculation of smoothness and gait profile indices
Movement smoothness was quantified using the Log Dimensionless Jerk (LDLJ) metric derived from the center of mass (COM) trajectory during a single gait cycle. The COM position signal was low-pass filtered using a zero-lag fourth-order Butterworth filter with a cut-off frequency of 10 Hz. COM velocity was subsequently obtained by differentiating the filtered position signal with respect to time, and jerk was estimated from the second derivative of velocity.
Movement smoothness was calculated according to the following equation
The experimental group participated in a six-week mind-body exercise program (three sessions per week, each lasting 60 minutes). Each session consisted of three parts: a warm-up (10 minutes), main exercises (40 minutes) including stretching, strengthening, and trunk control exercises in supine, sitting, and standing positions, and a cool-down (10 minutes) focusing on breathing and muscle relaxation. The intensity of the exercises was progressively increased from simple mat-based movements to combined exercises using an aerobic ball, resistance bands, and light weights.
The six-week intervention period was selected primarily based on participant availability, adherence considerations, and the feasibility of maintaining regular attendance among older adults. Although longer intervention durations have been reported in previous studies, the present protocol was designed to investigate the short-term effects of mind-body exercise on gait-related motor control parameters. Nevertheless, it should be acknowledged that a six-week duration may be insufficient to induce larger adaptations in sensitive movement control variables such as gait smoothness. The control group maintained their usual daily activities throughout the study period and were instructed not to participate in any additional structured exercise programs. After the six-week intervention period, the gait assessment was repeated for both groups following the same protocol used during the pre-test.
Results processing
Following data collection, initial processing was performed in Motive software, and the final analysis was conducted in MATLAB version 2021. The kinematic data were processed using a Gaussian low-pass filter with a cutoff frequency of 6 Hz to reduce signal noise and reconstruct occasional missing marker trajectories. After identifying the different gait phases using the positions of the markers attached to the foot, joint angles were calculated from the marker positions using an inverse kinematics approach. For each participant, a minimum of 10 complete gait cycles were analyzed. To improve measurement consistency, all data collection procedures, marker placements, and motion capture assessments were conducted by the same experienced examiner under identical laboratory conditions. Therefore, formal intra-rater and inter-rater reliability analyses (e.g., ICC) were not separately calculated in the present study.
The movements of the pelvis and hips in the three anatomical planes, along with the movements of the knees and ankles in the sagittal plane, and foot progression, constituted the 15 degrees of freedom that were estimated from the kinematic information. Subsequently, the values for the Smoothness Index and the Gait Profile Score were calculated.
Calculation of smoothness and gait profile indices
Movement smoothness was quantified using the Log Dimensionless Jerk (LDLJ) metric derived from the center of mass (COM) trajectory during a single gait cycle. The COM position signal was low-pass filtered using a zero-lag fourth-order Butterworth filter with a cut-off frequency of 10 Hz. COM velocity was subsequently obtained by differentiating the filtered position signal with respect to time, and jerk was estimated from the second derivative of velocity.
Movement smoothness was calculated according to the following equation
 |
Equation 1
In this equation,v t  represents the mediolateral COM velocity,
represents the mediolateral COM velocity, t  and
and t  denote the beginning and end of the gait cycle, respectively, and
denote the beginning and end of the gait cycle, respectively, and v peak  corresponds to the peak mediolateral COM velocity during the gait cycle. Higher LDLJ values indicate greater movement smoothness, whereas lower values reflect reduced smoothness and increased movement intermittency.
corresponds to the peak mediolateral COM velocity during the gait cycle. Higher LDLJ values indicate greater movement smoothness, whereas lower values reflect reduced smoothness and increased movement intermittency.
To calculate the Gait Profile Score (GPS), the deviation of the individual's walking pattern from a normal pattern was estimated. This index is based on calculating the mean Root Mean Square (RMS) error
between the subject's joint angles and reference values (normal gait pattern) throughout the gait cycle. Accordingly, for each joint degree of freedom, the Gait Variable Score (GVS) was first computed, which represents the extent of deviation of the joint angle from normal values for that degree of freedom. The GPS was then derived as the geometric mean of the GVS values across all degrees of freedom.
In Equation 2,GV S i  represents the Gait Variable Score for the i-th angular variable,
represents the Gait Variable Score for the i-th angular variable, N  denotes the number of data points in a single gait cycle,
denotes the number of data points in a single gait cycle, θ i k  represents the subject's joint angle at the k-th time point, and
represents the subject's joint angle at the k-th time point, and θ i k  is the joint angle from the normal gait pattern at the k-th time point.
is the joint angle from the normal gait pattern at the k-th time point.
Subsequently, the GPS for the 15 kinematic degrees of freedom was calculated according to Equation 3.
In this equation,
represents the mediolateral COM velocity, and denote the beginning and end of the gait cycle, respectively, and corresponds to the peak mediolateral COM velocity during the gait cycle. Higher LDLJ values indicate greater movement smoothness, whereas lower values reflect reduced smoothness and increased movement intermittency.To calculate the Gait Profile Score (GPS), the deviation of the individual's walking pattern from a normal pattern was estimated. This index is based on calculating the mean Root Mean Square (RMS) error
between the subject's joint angles and reference values (normal gait pattern) throughout the gait cycle. Accordingly, for each joint degree of freedom, the Gait Variable Score (GVS) was first computed, which represents the extent of deviation of the joint angle from normal values for that degree of freedom. The GPS was then derived as the geometric mean of the GVS values across all degrees of freedom.
In Equation 2,
represents the Gait Variable Score for the i-th angular variable, denotes the number of data points in a single gait cycle, represents the subject's joint angle at the k-th time point, and is the joint angle from the normal gait pattern at the k-th time point.Subsequently, the GPS for the 15 kinematic degrees of freedom was calculated according to Equation 3.
 |
Equation 2
Subsequently, the GPS for the 15 kinematic degrees of freedom was calculated according to Equation 3.
Subsequently, the GPS for the 15 kinematic degrees of freedom was calculated according to Equation 3.
 |
Equation 3
Statistical analysis
Data normality was assessed using the Shapiro–Wilk test separately for each variable, group, and measurement time point. Homogeneity of variances between groups was evaluated using Levene’s test. In addition, the assumption of sphericity for repeated measures was examined using Mauchly’s test. Because the study design included only two repeated measurements (pre-test and post-test), the assumption of sphericity was inherently satisfied; nevertheless, Greenhouse–Geisser corrected values were also inspected and yielded identical results.
Descriptive statistics are reported as mean ± standard deviation. To evaluate the effects of the intervention on movement smoothness and GPS, a two-way mixed-design repeated measures ANOVA was performed with time (pre-test vs. post-test) as the within-subject factor and group (experimental vs. control) as the between-subject factor. When significant main or interaction effects were identified, Bonferroni-adjusted pairwise comparisons were conducted for post-hoc analyses. Effect sizes were reported using partial eta squared (η²). Statistical analyses were performed using SPSS software (version 27), and the significance level was set at p < 0.05.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Yazd University (IR.YAZD.REC.1403.079). All participants provided written informed consent for participation in the study, data collection, and publication of their walking data and images.
Results
Participant demographic and baseline characteristics are presented in Table 1.
The results of the Shapiro–Wilk normality test demonstrated that all variables were normally distributed across groups and measurement time points (all p > 0.05), supporting the use of parametric statistical analyses. Furthermore, Mauchly’s test indicated that the assumption of sphericity was satisfied (W = 1.00). Levene’s test showed homogeneity of variances for movement smoothness at both pre-test and post-test assessments (p > 0.05). For GPS, homogeneity of variances was confirmed at pre-test (p = 0.835), whereas post-test values demonstrated unequal variances between groups (p = 0.011). Given the balanced sample sizes across groups, repeated-measures ANOVA is considered relatively robust to moderate violations of homogeneity of variance. Visual inspection of boxplots did not reveal any substantial outliers. Changes in movement smoothness and GPS across the experimental and control groups are illustrated in Figures 2 and 3, respectively. The results of the two-way mixed-design repeated measures ANOVA for both variables are presented in Table 2.
For movement smoothness, the mixed-design ANOVA revealed no significant main effect of time (F (1, 22) = 0.004, p = 0.952, η² = 0.000), indicating that smoothness values did not significantly change from pre-test to post-test across participants. Similarly, the main effect of group was not significant (F (1, 22) = 0.001, p = 0.981, η² = 0.000), suggesting no overall difference between the experimental and control groups. In addition, the interaction effect between time and group was not significant (F (1, 22) = 0.027, p = 0.871, η² = 0.001), indicating that the pattern of change over time was comparable between groups.
As illustrated in Figure 2, movement smoothness remained relatively stable across the intervention period in both groups.
For GPS, the mixed-design ANOVA demonstrated a significant main effect of time (F (1,22) = 13.318, p = 0.001, η² = 0.377), indicating an overall reduction in GPS values from pre-test to post-test. A significant main effect of group was also observed (F (1, 22) = 4.724, p = 0.041, η² = 0.177), suggesting overall differences between the experimental and control groups. Importantly, the interaction effect between time and group was significant (F (1, 22) = 6.798, p = 0.016, η² = 0.236), indicating that the magnitude of change over time differed between the two groups. Bonferroni-adjusted pairwise comparisons revealed that GPS values significantly decreased from pre-test to post-test (Mean Difference = 2.462, p = 0.001, 95% CI [1.063, 3.861]). In addition, the experimental group demonstrated significantly lower overall GPS values compared with the control group (Mean Difference = −3.663, p = 0.041, 95% CI [−7.158, −0.168]). As shown in Figure 3, participants in the experimental group exhibited a marked reduction in GPS following the six-week mind-body exercise intervention, whereas the control group demonstrated minimal change over time.
Statistical analysis
Data normality was assessed using the Shapiro–Wilk test separately for each variable, group, and measurement time point. Homogeneity of variances between groups was evaluated using Levene’s test. In addition, the assumption of sphericity for repeated measures was examined using Mauchly’s test. Because the study design included only two repeated measurements (pre-test and post-test), the assumption of sphericity was inherently satisfied; nevertheless, Greenhouse–Geisser corrected values were also inspected and yielded identical results.
Descriptive statistics are reported as mean ± standard deviation. To evaluate the effects of the intervention on movement smoothness and GPS, a two-way mixed-design repeated measures ANOVA was performed with time (pre-test vs. post-test) as the within-subject factor and group (experimental vs. control) as the between-subject factor. When significant main or interaction effects were identified, Bonferroni-adjusted pairwise comparisons were conducted for post-hoc analyses. Effect sizes were reported using partial eta squared (η²). Statistical analyses were performed using SPSS software (version 27), and the significance level was set at p < 0.05.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Yazd University (IR.YAZD.REC.1403.079). All participants provided written informed consent for participation in the study, data collection, and publication of their walking data and images.
Results
Participant demographic and baseline characteristics are presented in Table 1.
The results of the Shapiro–Wilk normality test demonstrated that all variables were normally distributed across groups and measurement time points (all p > 0.05), supporting the use of parametric statistical analyses. Furthermore, Mauchly’s test indicated that the assumption of sphericity was satisfied (W = 1.00). Levene’s test showed homogeneity of variances for movement smoothness at both pre-test and post-test assessments (p > 0.05). For GPS, homogeneity of variances was confirmed at pre-test (p = 0.835), whereas post-test values demonstrated unequal variances between groups (p = 0.011). Given the balanced sample sizes across groups, repeated-measures ANOVA is considered relatively robust to moderate violations of homogeneity of variance. Visual inspection of boxplots did not reveal any substantial outliers. Changes in movement smoothness and GPS across the experimental and control groups are illustrated in Figures 2 and 3, respectively. The results of the two-way mixed-design repeated measures ANOVA for both variables are presented in Table 2.
For movement smoothness, the mixed-design ANOVA revealed no significant main effect of time (F (1, 22) = 0.004, p = 0.952, η² = 0.000), indicating that smoothness values did not significantly change from pre-test to post-test across participants. Similarly, the main effect of group was not significant (F (1, 22) = 0.001, p = 0.981, η² = 0.000), suggesting no overall difference between the experimental and control groups. In addition, the interaction effect between time and group was not significant (F (1, 22) = 0.027, p = 0.871, η² = 0.001), indicating that the pattern of change over time was comparable between groups.
As illustrated in Figure 2, movement smoothness remained relatively stable across the intervention period in both groups.
For GPS, the mixed-design ANOVA demonstrated a significant main effect of time (F (1,22) = 13.318, p = 0.001, η² = 0.377), indicating an overall reduction in GPS values from pre-test to post-test. A significant main effect of group was also observed (F (1, 22) = 4.724, p = 0.041, η² = 0.177), suggesting overall differences between the experimental and control groups. Importantly, the interaction effect between time and group was significant (F (1, 22) = 6.798, p = 0.016, η² = 0.236), indicating that the magnitude of change over time differed between the two groups. Bonferroni-adjusted pairwise comparisons revealed that GPS values significantly decreased from pre-test to post-test (Mean Difference = 2.462, p = 0.001, 95% CI [1.063, 3.861]). In addition, the experimental group demonstrated significantly lower overall GPS values compared with the control group (Mean Difference = −3.663, p = 0.041, 95% CI [−7.158, −0.168]). As shown in Figure 3, participants in the experimental group exhibited a marked reduction in GPS following the six-week mind-body exercise intervention, whereas the control group demonstrated minimal change over time.
Figure 1. A participant performing the walking task on the treadmill
Table 1. Descriptive characteristics of participants (Mean ± SD)
| Characteristic | Experimental group (Mean ± SD) |
Control group (Mean ± SD) |
| Age (years) | 62.5 ± 4.7 | 65.7 ± 4.6 |
| Height (cm) | 152.1 ± 8.9 | 154.9 ± 5.6 |
| Body Mass (kg) | 66.3 ± 14.6 | 65.6 ± 11.0 |
Table 2. Results of the two-way mixed-design repeated measures ANOVA for movement smoothness and gait profile score
| Variable | Effect | Mean square | F | df | p-value | η² |
| Movement Smoothness |
Group | 0.001 | 0.001 | 1, 22 | 0.981 | 0.000 |
| Time | 0.002 | 0.004 | 1, 22 | 0.952 | 0.000 | |
| Group × Time | 0.011 | 0.027 | 1, 22 | 0.871 | 0.001 | |
| Gait Profile Score |
Group | 161.020 | 4.724 | 1, 22 | 0.041 | 0.177 |
| Time | 72.719 | 13.318 | 1, 22 | 0.001 | 0.377 | |
| Group × Time | 37.115 | 6.798 | 1, 22 | 0.016 | 0.236 |
Figure 2. Movement smoothness values across pre-test and post-test assessments in the experimental and control groups. Bars represent mean values, error bars indicate standard deviation, and scatter points represent individual participant data.
Figure 3. Gait Profile Score across pre-test and post-test assessments in the experimental and control groups. Bars represent mean values, error bars indicate standard deviation, and scatter points represent individual participant data.
Discussion
The aim of this study was to investigate the effects of six weeks of mind-body exercise on qualitative gait indices, including movement smoothness and the GPS, in elderly women. The findings of the present study indicated that while these exercises did not have a significant effect on the movement smoothness index, they led to a significant reduction in the GPS. This reduction signifies a qualitative improvement in the walking pattern, bringing it closer to the normal pattern.
Data analysis revealed that the GPS in the experimental group decreased significantly after the intervention. This finding suggests that the exercises shifted the movement pattern of the elderly women toward a more normal and optimized gait pattern. To the best of our knowledge, no study has directly investigated the effect of exercise programs on the GPS in an elderly population. Only one study with a similar approach was conducted by Pao et al., on individuals with Parkinson's disease. That study demonstrated that integrated rehabilitation with auditory cues led to better coordination between the hip, knee, and ankle joints, an improved overall movement pattern, and ultimately, a reduction in the GPS in these patients (17). In contrast, previous research in the field of aging has primarily focused on the impact of exercises such as Pilates on indices like functional mobility, balance, and spatial gait parameters, reporting improvements in these variables following intervention (18, 19).
Several mechanisms may underlie the effectiveness of Pilates exercises in improving function in older adults. the most important among these are enhancement of core muscle strength (20), increased pelvic stability (21), improved range of motion and flexibility, and promotion of neuromuscular coordination. The core muscles are primarily responsible for maintaining trunk stability and improving pelvis-trunk coordination. The age-related weakening of these muscles can directly lead to impaired functional balance and reduced mobility (22). Pilates exercises, with their specific emphasis on strengthening the core muscles (including the abdominal, back, and pelvic muscles), increase the strength and endurance of this musculature. This, in turn, leads to better stability of the core region and superior control of pelvic movements during the various phases of gait. Such improved stability facilitates the execution of a more efficient movement pattern with less deviation from the norm.
In line with these findings, a study by Ferreira et al., on individuals with diabetic neuropathy demonstrated that the GPS is highly correlated with pelvic kinematic parameters, particularly pelvic rotation (23). Therefore, it appears that improving pelvic stability and reducing its excessive rotation through Pilates exercises is a key mechanism in optimizing the walking pattern and, consequently, reducing the GPS. Furthermore, performing Pilates exercises through a full range of motion, combined with stretching the muscles around the pelvis, contributes to improving joint range of motion (24) and achieving better kinematic alignment of the limbs. There is also evidence suggesting that Pilates can induce morphological changes in muscle fibers, leading to tissue adaptations and ultimately increased flexibility (25).
The integrative nature of Pilates exercises—encompassing mental focus, precise motor control, and mindful breathing—can enhance neuromuscular communication and increase proprioceptive acuity. By inducing beneficial adaptations at the neuromuscular level and facilitating cortical remapping, these exercises contribute to improved sensorimotor system function (26). This level of enhanced coordination enables more precise control of joint angles and more optimal movement synchronization throughout the gait cycle, which is directly reflected in the reduction of the GPS. Furthermore, the present finding of an improved GPS aligns with studies demonstrating that other mind-body exercises such as Tai Chi, yoga, and resistance training can also reduce gait dysfunction and increase walking stability, thereby lowering the risk of falls in the elderly (27).
Data analysis indicated that the Pilates training did not have a significant effect on the movement smoothness index. To the best of our knowledge, no study has directly investigated the effect of exercise training on this specific index in an elderly population. In a related study, Antonelli et al., by comparing the movement smoothness index between older adults and younger individuals, found that the aging process alone might have a lesser impact on gait smoothness, suggesting that other factors such as cognitive impairments play a more prominent role (28). This finding could partially explain why the movement smoothness index of our participants was not substantially impaired at baseline and, consequently, why the exercise intervention failed to induce a noticeable change. On the other hand, the movement smoothness index, calculated based on angular jerk, is
likely a metric with very high sensitivity to subtle alterations in motor control. It seems that the current six-week training period was insufficient to induce measurable changes in such a sensitive parameter. Furthermore, the controlled and slow-paced nature of Pilates exercises might not have fully transferred to the dynamic and automatic task of walking at a self-selected speed. This finding underscores the necessity for employing longer training durations or utilizing alternative metrics to assess movement smoothness in future studies.
Conclusion
The findings indicate that, although six weeks of Pilates training did not significantly affect the movement smoothness index derived from angular jerk, it successfully improved the qualitative walking pattern of elderly women. This improvement was demonstrated by a significant reduction in the overall GPS. This enhancement signifies a more efficient gait pattern that more closely resembles the normal pattern. Specifically, the observed improvement in the GPS can be primarily attributed to the strengthening of core muscles, increased pelvic stability, and enhanced neuromuscular coordination, which are considered the primary mechanisms through which Pilates exercises exert their effects. Given that the Gait Profile Score is a sensitive and comprehensive index of movement pattern deviation, its reduction may translate to a decreased risk of falls and an enhanced quality of life in the elderly population.
Study limitations
This study has several limitations that should be acknowledged. First, the relatively small sample size and inclusion of only elderly women restrict the generalizability of the findings. Second, the six-week intervention period may not have been long enough to induce measurable changes in movement smoothness. Third, gait analysis was performed under controlled treadmill conditions, which might differ from natural walking. Furthermore, potential confounding factors such as habitual physical activity and nutrition were not controlled. Future studies with larger and more diverse samples, longer intervention durations, and additional kinetic or electromyographic assessments are recommended to confirm and extend these findings.
Conflict of interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-public sectors.
Acknowledgments
We would like to thank all participants in this research.
Authors’ contributions
Author 1 (E.D.N): Conceptualization, Investigation, Curated the data, drafted the initial version of the manuscript. Author 2 (M.H.L): Conceptualization, Data Curation, and developed the research plan and methodology, conducted the statistical analysis, Writing – Original Draft. Author 3 (F.Z.B): Provided critical revisions and feedback on the manuscript, Writing – Review & Editing.
Reference
Data analysis revealed that the GPS in the experimental group decreased significantly after the intervention. This finding suggests that the exercises shifted the movement pattern of the elderly women toward a more normal and optimized gait pattern. To the best of our knowledge, no study has directly investigated the effect of exercise programs on the GPS in an elderly population. Only one study with a similar approach was conducted by Pao et al., on individuals with Parkinson's disease. That study demonstrated that integrated rehabilitation with auditory cues led to better coordination between the hip, knee, and ankle joints, an improved overall movement pattern, and ultimately, a reduction in the GPS in these patients (17). In contrast, previous research in the field of aging has primarily focused on the impact of exercises such as Pilates on indices like functional mobility, balance, and spatial gait parameters, reporting improvements in these variables following intervention (18, 19).
Several mechanisms may underlie the effectiveness of Pilates exercises in improving function in older adults. the most important among these are enhancement of core muscle strength (20), increased pelvic stability (21), improved range of motion and flexibility, and promotion of neuromuscular coordination. The core muscles are primarily responsible for maintaining trunk stability and improving pelvis-trunk coordination. The age-related weakening of these muscles can directly lead to impaired functional balance and reduced mobility (22). Pilates exercises, with their specific emphasis on strengthening the core muscles (including the abdominal, back, and pelvic muscles), increase the strength and endurance of this musculature. This, in turn, leads to better stability of the core region and superior control of pelvic movements during the various phases of gait. Such improved stability facilitates the execution of a more efficient movement pattern with less deviation from the norm.
In line with these findings, a study by Ferreira et al., on individuals with diabetic neuropathy demonstrated that the GPS is highly correlated with pelvic kinematic parameters, particularly pelvic rotation (23). Therefore, it appears that improving pelvic stability and reducing its excessive rotation through Pilates exercises is a key mechanism in optimizing the walking pattern and, consequently, reducing the GPS. Furthermore, performing Pilates exercises through a full range of motion, combined with stretching the muscles around the pelvis, contributes to improving joint range of motion (24) and achieving better kinematic alignment of the limbs. There is also evidence suggesting that Pilates can induce morphological changes in muscle fibers, leading to tissue adaptations and ultimately increased flexibility (25).
The integrative nature of Pilates exercises—encompassing mental focus, precise motor control, and mindful breathing—can enhance neuromuscular communication and increase proprioceptive acuity. By inducing beneficial adaptations at the neuromuscular level and facilitating cortical remapping, these exercises contribute to improved sensorimotor system function (26). This level of enhanced coordination enables more precise control of joint angles and more optimal movement synchronization throughout the gait cycle, which is directly reflected in the reduction of the GPS. Furthermore, the present finding of an improved GPS aligns with studies demonstrating that other mind-body exercises such as Tai Chi, yoga, and resistance training can also reduce gait dysfunction and increase walking stability, thereby lowering the risk of falls in the elderly (27).
Data analysis indicated that the Pilates training did not have a significant effect on the movement smoothness index. To the best of our knowledge, no study has directly investigated the effect of exercise training on this specific index in an elderly population. In a related study, Antonelli et al., by comparing the movement smoothness index between older adults and younger individuals, found that the aging process alone might have a lesser impact on gait smoothness, suggesting that other factors such as cognitive impairments play a more prominent role (28). This finding could partially explain why the movement smoothness index of our participants was not substantially impaired at baseline and, consequently, why the exercise intervention failed to induce a noticeable change. On the other hand, the movement smoothness index, calculated based on angular jerk, is
likely a metric with very high sensitivity to subtle alterations in motor control. It seems that the current six-week training period was insufficient to induce measurable changes in such a sensitive parameter. Furthermore, the controlled and slow-paced nature of Pilates exercises might not have fully transferred to the dynamic and automatic task of walking at a self-selected speed. This finding underscores the necessity for employing longer training durations or utilizing alternative metrics to assess movement smoothness in future studies.
Conclusion
The findings indicate that, although six weeks of Pilates training did not significantly affect the movement smoothness index derived from angular jerk, it successfully improved the qualitative walking pattern of elderly women. This improvement was demonstrated by a significant reduction in the overall GPS. This enhancement signifies a more efficient gait pattern that more closely resembles the normal pattern. Specifically, the observed improvement in the GPS can be primarily attributed to the strengthening of core muscles, increased pelvic stability, and enhanced neuromuscular coordination, which are considered the primary mechanisms through which Pilates exercises exert their effects. Given that the Gait Profile Score is a sensitive and comprehensive index of movement pattern deviation, its reduction may translate to a decreased risk of falls and an enhanced quality of life in the elderly population.
Study limitations
This study has several limitations that should be acknowledged. First, the relatively small sample size and inclusion of only elderly women restrict the generalizability of the findings. Second, the six-week intervention period may not have been long enough to induce measurable changes in movement smoothness. Third, gait analysis was performed under controlled treadmill conditions, which might differ from natural walking. Furthermore, potential confounding factors such as habitual physical activity and nutrition were not controlled. Future studies with larger and more diverse samples, longer intervention durations, and additional kinetic or electromyographic assessments are recommended to confirm and extend these findings.
Conflict of interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-public sectors.
Acknowledgments
We would like to thank all participants in this research.
Authors’ contributions
Author 1 (E.D.N): Conceptualization, Investigation, Curated the data, drafted the initial version of the manuscript. Author 2 (M.H.L): Conceptualization, Data Curation, and developed the research plan and methodology, conducted the statistical analysis, Writing – Original Draft. Author 3 (F.Z.B): Provided critical revisions and feedback on the manuscript, Writing – Review & Editing.
Reference
- Lally F, Crome P. Understanding frailty. Postgraduate Medical Journal. 2007; 83(975): 16-20.
- Marzuca-Nassr GN, Alegría-Molina A, SanMartín-Calísto Y, Artigas-Arias M, Huard N, Sapunar J, et al. Muscle mass and strength gains following resistance exercise training in older adults 65–75 years and older adults above 85 years. International Journal of Sport Nutrition and Exercise Metabolism. 2023; 34(1): 11-9.
- Guirguis-Blake JM, Perdue LA, Coppola EL, Bean SL. Interventions to prevent falls in older adults: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2018: 332(1): 58-69.
- Fujita K, Umegaki H, Makino T, Uemura K, Hayashi T, Inoue A, et al. Short-and long-term effects of different exercise programs on the gait performance of older adults with subjective cognitive decline: A randomized controlled trial. Experimental Gerontology. 2021. 156: 111590.
- Wang X, O’Dwyer N, Halaki M. A review on the coordinative structure of human walking and the application of principal component analysis. Neural Regeneration Research. 2013; 8(7): 662-70.
- Anaya-Campos LE, Sánchez-Fernández LP, Quiñones-Urióstegui I. Motion smoothness analysis of the gait cycle, segmented by stride and associated with the inertial sensors’ locations. Sensors. 2025; 25(2): 1-18.
- Hostler D, Schwob J, Schlader ZJ, Cavuoto L. Heat stress increases movement jerk during physical exertion. Frontiers in Physiology. 2021; 12: 1-6.
- Prince F, Corriveau H, Hébert R, Winter DA. Gait in the elderly. Gait & Posture. 1997; 5(2): 128-35.
- Pau M, Mulas I, Putzu V, Asoni G, Viale D, Mameli I, et al. Smoothness of gait in healthy and cognitively impaired individuals: a study on Italian elderly using wearable inertial sensor. Sensors. 2020; 20(12): 3577.
- Irez GB, Ozdemir RA, Evin R, Irez SG, Korkusuz F. Integrating Pilates exercise into an exercise program for 65+ year-old women to reduce falls. Journal of Sports Science & Medicine. 2011; 10(1): 105-11.
- Kloubec JA. Pilates for improvement of muscle endurance, flexibility, balance, and posture. The Journal of Strength & Conditioning Research. 2010; 24(3): 661-7.
- Aibar-Almazán A, Martínez-Amat A, Cruz-Díaz D, de la Torre-Cruz MJ, Jiménez-García JD, Zagalaz-Anula N, et al. The influence of Pilates exercises on body composition, muscle strength, and gait speed in community-dwelling older women: a randomized controlled trial. The Journal of Strength & Conditioning Research. 2022; 36(8): 2298-305.
- Meikis L, Wicker P, Donath L. Effects of Pilates training on physiological and psychological health parameters in healthy older adults and in older adults with clinical conditions over 55 years: a meta-analytical review. Frontiers in Neurology. 2021; 12: 1-17.
- Buisseret F, Catinus L, Grenard R, Jojczyk L, Fievez D, Barvaux V, et al. Timed up and go and six-minute walking tests with wearable inertial sensor: one step further for the prediction of the risk of fall in elderly nursing home people. Sensors. 2020; 20(11): 1-16.
- Shanahan CJ, Boonstra FM, Cofré Lizama LE, Strik M, Moffat BA, Khan F, et al. Technologies for advanced gait and balance assessments in people with multiple sclerosis. Frontiers in Neurology. 2018; 8: 1-10.
- Sasagawa S, Arakawa A, Furuyama A, Matsumoto Y. Age-related changes in static balance in older women aged in their early sixties to their late eighties: different aging patterns in the anterior–posterior and mediolateral directions. Frontiers in Aging Neuroscience. 2024; 16: 1-9.
- Pau M, Corona F, Pili R, Casula C, Sors F, Agostini T, et al. Effects of physical rehabilitation integrated with rhythmic auditory stimulation on spatio-temporal and kinematic parameters of gait in Parkinson’s disease. Frontiers in Neurology. 2016; 7: 1-12.
- da Silva LD, Shiel A, McIntosh C. Effects of Pilates on the risk of falls, gait, balance and functional mobility in healthy older adults: A randomised controlled trial. Journal of Bodywork and Movement Therapies. 2022; 30: 30-41.
- Fernández-Rodríguez R, Álvarez-Bueno C, Ferri-Morales A, Torres-Costoso A, Pozuelo-Carrascosa DP, Martínez-Vizcaíno V. Pilates improves physical performance and decreases risk of falls in older adults: a systematic review and meta-analysis. Physiotherapy. 2021; 112: 163-77.
- Ko HS, Jung HU, Park TY, Song JK, Wang J, Jung HC. Comparisons of functional movements and core muscle activity in women according to Pilates proficiency. Frontiers in Physiology. 2024; 15: 1-11.
- Işık Eİ, Başar S. Pilates training in the elderly. International Journal of Academic Medicine and Pharmacy. 2021; 3(3): 277-80.
- Paquette C, Paquet N, Fung J. Aging affects coordination of rapid head motions with trunk and pelvis movements during standing and walking. Gait & Posture. 2006; 24(1): 62-69.
- Ferreira JS, Cruvinel-Júnior RH, Marcos Duarte M, Isabel CN, Sacco ICN. Gait Profile Scores and their correlation with clinical outcomes in individuals with diabetic neuropathy: a cross-sectional study with 102 patients. Gait & Posture. 2025; 122: 240-6.
- Choi W, Joo Y, Lee S. Pilates exercise focused on ankle movements for improving gait ability in older women. Journal of Women & Aging. 2021; 33(1): 30-40.
- Geremia JM, Iskiewicz MM, Marschner RA, Lehnen TE, Lehnen AM. Effect of a physical training program using the Pilates method on flexibility in elderly subjects. Age. 2015; 37(6):1-12.
- Carrasco-Poyatos M, Rubio-Arias JA, Ballesta-García I, Ramos-Campo DJ. Pilates vs. muscular training in older women. Effects in functional factors and the cognitive interaction: A randomized controlled trial. Physiology & behavior. 2019; 201: 157-64.
- Mahajan L, Mahajan P, Shinde M, Prakash A. Effect of tai chi exercise versus pilates on dynamic balance and gait in elderly-a comparative study. International Journal of Health Sciences and Research. 2022; 12(7): 200-13.
- Antonelli M, Caselli E, Gastaldi L. Comparison of gait smoothness metrics in healthy elderly and young people. Applied Sciences. 2024; 14(2): 911.
Type of Study: Research |
Subject:
General
Received: 2025/11/15 | Accepted: 2026/06/10 | Published: 2026/06/20
Received: 2025/11/15 | Accepted: 2026/06/10 | Published: 2026/06/20
References
1. Lally F, Crome P. Understanding frailty. Postgraduate Medical Journal. 2007; 83(975): 16-20.
2. Marzuca-Nassr GN, Alegría-Molina A, SanMartín-Calísto Y, Artigas-Arias M, Huard N, Sapunar J, et al. Muscle mass and strength gains following resistance exercise training in older adults 65–75 years and older adults above 85 years. International Journal of Sport Nutrition and Exercise Metabolism. 2023; 34(1): 11-9.
3. Guirguis-Blake JM, Perdue LA, Coppola EL, Bean SL. Interventions to prevent falls in older adults: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2018: 332(1): 58-69.
4. Fujita K, Umegaki H, Makino T, Uemura K, Hayashi T, Inoue A, et al. Short-and long-term effects of different exercise programs on the gait performance of older adults with subjective cognitive decline: A randomized controlled trial. Experimental Gerontology. 2021. 156: 111590.
5. Wang X, O’Dwyer N, Halaki M. A review on the coordinative structure of human walking and the application of principal component analysis. Neural Regeneration Research. 2013; 8(7): 662-70.
6. Anaya-Campos LE, Sánchez-Fernández LP, Quiñones-Urióstegui I. Motion smoothness analysis of the gait cycle, segmented by stride and associated with the inertial sensors’ locations. Sensors. 2025; 25(2): 1-18.
7. Hostler D, Schwob J, Schlader ZJ, Cavuoto L. Heat stress increases movement jerk during physical exertion. Frontiers in Physiology. 2021; 12: 1-6.
8. Prince F, Corriveau H, Hébert R, Winter DA. Gait in the elderly. Gait & Posture. 1997; 5(2): 128-35.
9. Pau M, Mulas I, Putzu V, Asoni G, Viale D, Mameli I, et al. Smoothness of gait in healthy and cognitively impaired individuals: a study on Italian elderly using wearable inertial sensor. Sensors. 2020; 20(12): 3577.
10. Irez GB, Ozdemir RA, Evin R, Irez SG, Korkusuz F. Integrating Pilates exercise into an exercise program for 65+ year-old women to reduce falls. Journal of Sports Science & Medicine. 2011; 10(1): 105-11.
11. Kloubec JA. Pilates for improvement of muscle endurance, flexibility, balance, and posture. The Journal of Strength & Conditioning Research. 2010; 24(3): 661-7.
12. Aibar-Almazán A, Martínez-Amat A, Cruz-Díaz D, de la Torre-Cruz MJ, Jiménez-García JD, Zagalaz-Anula N, et al. The influence of Pilates exercises on body composition, muscle strength, and gait speed in community-dwelling older women: a randomized controlled trial. The Journal of Strength & Conditioning Research. 2022; 36(8): 2298-305.
13. Meikis L, Wicker P, Donath L. Effects of Pilates training on physiological and psychological health parameters in healthy older adults and in older adults with clinical conditions over 55 years: a meta-analytical review. Frontiers in Neurology. 2021; 12: 1-17.
14. Buisseret F, Catinus L, Grenard R, Jojczyk L, Fievez D, Barvaux V, et al. Timed up and go and six-minute walking tests with wearable inertial sensor: one step further for the prediction of the risk of fall in elderly nursing home people. Sensors. 2020; 20(11): 1-16.
15. Shanahan CJ, Boonstra FM, Cofré Lizama LE, Strik M, Moffat BA, Khan F, et al. Technologies for advanced gait and balance assessments in people with multiple sclerosis. Frontiers in Neurology. 2018; 8: 1-10.
16. Sasagawa S, Arakawa A, Furuyama A, Matsumoto Y. Age-related changes in static balance in older women aged in their early sixties to their late eighties: different aging patterns in the anterior–posterior and mediolateral directions. Frontiers in Aging Neuroscience. 2024; 16: 1-9.
17. Pau M, Corona F, Pili R, Casula C, Sors F, Agostini T, et al. Effects of physical rehabilitation integrated with rhythmic auditory stimulation on spatio-temporal and kinematic parameters of gait in Parkinson’s disease. Frontiers in Neurology. 2016; 7: 1-12.
18. da Silva LD, Shiel A, McIntosh C. Effects of Pilates on the risk of falls, gait, balance and functional mobility in healthy older adults: A randomised controlled trial. Journal of Bodywork and Movement Therapies. 2022; 30: 30-41.
19. Fernández-Rodríguez R, Álvarez-Bueno C, Ferri-Morales A, Torres-Costoso A, Pozuelo-Carrascosa DP, Martínez-Vizcaíno V. Pilates improves physical performance and decreases risk of falls in older adults: a systematic review and meta-analysis. Physiotherapy. 2021; 112: 163-77.
20. Ko HS, Jung HU, Park TY, Song JK, Wang J, Jung HC. Comparisons of functional movements and core muscle activity in women according to Pilates proficiency. Frontiers in Physiology. 2024; 15: 1-11.
21. Işık Eİ, Başar S. Pilates training in the elderly. International Journal of Academic Medicine and Pharmacy. 2021; 3(3): 277-80.
22. Paquette C, Paquet N, Fung J. Aging affects coordination of rapid head motions with trunk and pelvis movements during standing and walking. Gait & Posture. 2006; 24(1): 62-69.
23. Ferreira JS, Cruvinel-Júnior RH, Marcos Duarte M, Isabel CN, Sacco ICN. Gait Profile Scores and their correlation with clinical outcomes in individuals with diabetic neuropathy: a cross-sectional study with 102 patients. Gait & Posture. 2025; 122: 240-6.
24. Choi W, Joo Y, Lee S. Pilates exercise focused on ankle movements for improving gait ability in older women. Journal of Women & Aging. 2021; 33(1): 30-40.
25. Geremia JM, Iskiewicz MM, Marschner RA, Lehnen TE, Lehnen AM. Effect of a physical training program using the Pilates method on flexibility in elderly subjects. Age. 2015; 37(6):1-12.
26. Carrasco-Poyatos M, Rubio-Arias JA, Ballesta-García I, Ramos-Campo DJ. Pilates vs. muscular training in older women. Effects in functional factors and the cognitive interaction: A randomized controlled trial. Physiology & behavior. 2019; 201: 157-64.
27. Mahajan L, Mahajan P, Shinde M, Prakash A. Effect of tai chi exercise versus pilates on dynamic balance and gait in elderly-a comparative study. International Journal of Health Sciences and Research. 2022; 12(7): 200-13.
28. Antonelli M, Caselli E, Gastaldi L. Comparison of gait smoothness metrics in healthy elderly and young people. Applied Sciences. 2024; 14(2): 911.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
