

Volume 12, Issue 1 (June 2026)
Elderly Health Journal 2026, 12(1): 23-33 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Maleki S, Ghafori E, Babalou K, Gorbanalipour M. The Role of Health Anxiety in Illness Perception: The Mediating Effect of Bodily Symptom Vigilance among Elderly Patients Attending Medical Clinics in Urmia. Elderly Health Journal 2026; 12 (1) :23-33
URL: http://ehj.ssu.ac.ir/article-1-377-en.html
URL: http://ehj.ssu.ac.ir/article-1-377-en.html



Department of Psychology, Faculty of Psychology and Educational Sciences, Islamic Azad University, Khoy Branch, Khoy, Iran , masoudqorbanalipour@gmail.com
Full-Text [PDF 523 kb]
(34 Downloads)
| Abstract (HTML) (153 Views)
Table 1. Demographic characteristics of the participants and descriptive statistics of age
Table 2. Correlation matrix of study variables
p < 0.01
Table 3. Measurement model fit indices (Reliability indicators)
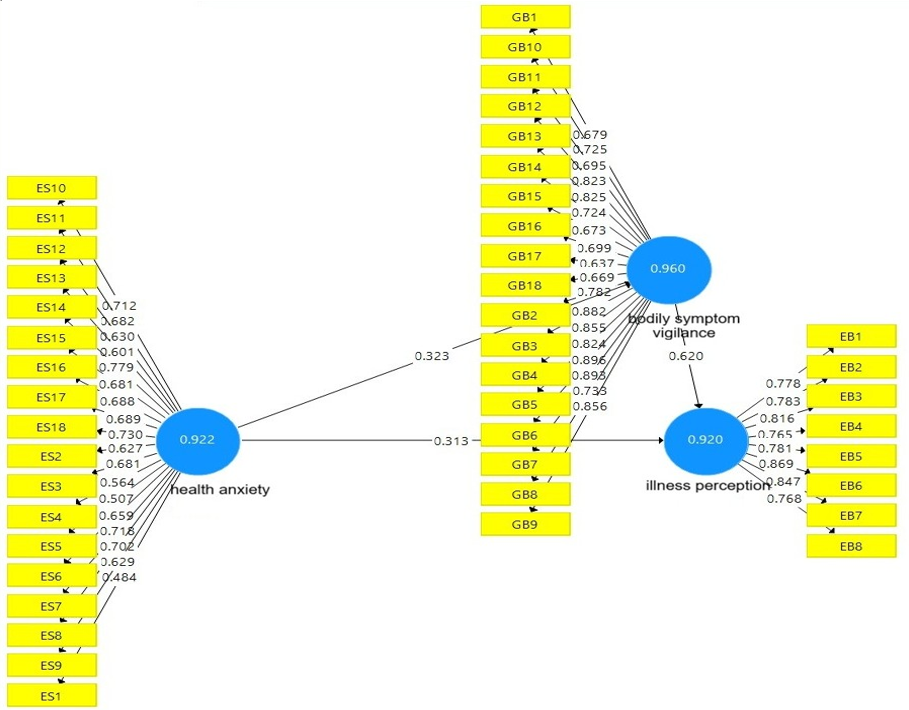
Figure 1. Structural equation model of the relationships among health anxiety, bodily symptom vigilance, and illness perception
Full-Text: (12 Views)
The Role of Health Anxiety in Illness Perception: The Mediating Effect of Bodily Symptom Vigilance among Elderly Patients Attending Medical Clinics in Urmia
Shayan Maleki 1, Elahe Ghafouri 2, Kosar Babalou 3, Masoud Gorbanalipour 1*
* Corresponding Author: Department of Psychology, Faculty of Psychology and Educational Sciences, Islamic Azad University, Khoy Branch, Khoy, Iran. Tel: +98 9141633787, Email address: masoudqorbanalipour@gmail.com
Shayan Maleki 1, Elahe Ghafouri 2, Kosar Babalou 3, Masoud Gorbanalipour 1*
- Department of Psychology, Faculty of Psychology and Educational Sciences, Islamic Azad University, Khoy Branch, Khoy, Iran
- Department of Educational Psychology, Islamic Azad University, Urmia Branch, Urmia, Iran
- Department of Clinical Psychology, Islamic Azad University, Urmia Branch, Urmia, Iran
* Corresponding Author: Department of Psychology, Faculty of Psychology and Educational Sciences, Islamic Azad University, Khoy Branch, Khoy, Iran. Tel: +98 9141633787, Email address: masoudqorbanalipour@gmail.com
| A B S T R A C T | |
| Article history Received 21 Apr 2026 Accepted 8 Jun 2026 |
Introduction: Health anxiety is recognized as an important psychological factor influencing individuals’ perception of illness, particularly among older adults. However, the mechanisms underlying this relationship, especially the mediating role of bodily symptom vigilance, remain insufficiently explored. The present study aimed to investigate the role of health anxiety in illness perception, emphasizing the mediating effect of bodily symptom vigilance among elderly individuals attending medical clinics in Urmia. Methods: This fundamental study employed a descriptive-correlational design using structural equation modeling. The statistical population included individuals aged 60 years and older who visited medical centers in Urmia in 2024. A convenience sample of 200 participants was selected. Data were collected using the Health Anxiety Inventory, the Brief Illness Perception Questionnaire, and the Body Vigilance Scale. Data analysis was performed using SPSS and SmartPLS software. Results: Health anxiety significantly predicted illness perception both directly (β = 0.313, t = 5.04, p < 0.001) and indirectly through bodily symptom vigilance (β = 0.200, t = 4.26, p < 0.001). Health anxiety also significantly predicted bodily symptom vigilance (β = 0.323, t = 5.27, p < 0.001), while bodily symptom vigilance significantly predicted illness perception (β = 0.620, t = 10.60, p < 0.001). Model fit indices indicated an acceptable fit of the proposed model (SRMR = 0.089, NFI = 0.891). Conclusion: Health anxiety and heightened bodily vigilance play a crucial role in shaping illness perception among older adults. These findings highlight the importance of addressing psychological factors in developing mental health policies and interventions for the elderly population. Keywords: Health Anxiety, Disease Perception, Bodily Symptom Vigilance |
Citation: Maleki SH, Ghafouri E, Babalou K, Gorbanalipour M. The role of health anxiety in illness perception: the mediating effect of bodily symptom vigilance among elderly patients attending medical clinics in Urmia. Elderly Health Journal. 2026; 12(1): 23-33. |
Introduction
Aging is a phenomenon caused by biological, physiological, biochemical, and anatomical changes in the body’s cells (1). These changes gradually affect cellular function and, in terms of age, are defined as the transition beyond 60 years of age (2, 3). Aging has various consequences across physical, social, economic, familial, and psychological dimensions (4, 5). In examining psychological problems among older adults, feelings of loneliness, boredom, irritability, emptiness, anxiety and worry, insomnia, fatigue, and exhaustion are among the most prominent issues (6). In addition, entering old age can trigger psychological consequences, including health anxiety and fear of illness (7). Due to their physical condition, older adults are at higher risk of developing illnesses and are more likely to experience somatic symptoms and perceive themselves as ill (8). Illness perception plays an important role in an individual’s behavior, adaptation to illness, self-management of the disease, and ultimately its outcome (9). Illness perception refers to the beliefs and mental images that patients hold about their illness, and this cognitive representation influences their adaptation to the disease as well as their psychological state and anxiety levels (10). Illness perception consists of five dimensions: identity (symptoms), timeline (duration of illness), cause, consequences/outcomes, and controllability /treatability (11). It also refers to the patient’s organized cognitive representation of their illness and their beliefs about different aspects of their new health condition (12). Based on Leventhal’s self-regulation model, patients determine their behavioral and emotional responses to illness based on their perception of symptoms, beliefs about treatments, perceived impact of the illness on overall life, expected duration of the illness, and beliefs about controllability and cyclicality of the disease and its treatment (13). In other words, illness perception helps identify factors influencing adaptation to and acceptance of the disease (14) and is associated with patients’ quality of life (15).
Research shows that illness perception influences individuals’ self-care behaviors (16, 17). Studies have demonstrated that illness perception is one of the most important predictors of low-level adaptation outcomes, including social dysfunction, fatigue, anxiety, depression, and self-esteem (18). Furthermore, research indicates that illness perception has an impact on individuals’ mental health and psychological quality of life (19). In addition, a study found a significant relationship between illness perception, quality of life, and optimism in patients (20). One of the issues that older adults—especially those who are aware of having a disease or are concerned about becoming ill—struggle with is health anxiety (21). This is because older adults, due to aging and reduced immune function, often experience numerous thoughts and concerns about their health (22).
Health anxiety, or illness anxiety disorder, was first introduced in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM) 5 under the category of somatic symptom disorders. Previously, in DSM-III and DSM-IV, it was referred to as hypochondriasis (23). This disorder creates a chronic, episodic, and recurrent condition that often begins in early adulthood and worsens with age, affecting men and women equally. Health anxiety refers to a condition characterized by the misinterpretation of bodily sensations or physical changes as signs of a serious illness. Individuals affected by health anxiety are preoccupied with the belief that they are currently suffering from a physical disease (24). Evidence suggests that health anxiety has a dimensional structure, ranging from the absence of concern about one’s health at one end to excessive anxiety about health at the other (25). Health anxiety differs from general anxiety because it involves irrational concerns that physical symptoms indicate the presence of a serious illness (21, 26). Salkovskis and Warwick (27) described four dysfunctional health-related beliefs that are particularly important for understanding health anxiety: the likelihood of having or developing a serious illness, fear of illness, perceived inability to cope with illness, and the belief that medical services are insufficient for effective treatment.
In its severe form, health anxiety has a significant long-term impact on individuals’ self-rated physical and mental health functioning, as well as on healthcare costs (28). In this disorder, physical symptoms may be absent or very mild; therefore, the individual’s distress is not primarily caused by somatic symptoms, but rather by anxiety and worry about the causes and consequences of an undiagnosed illness (29-31). As a result of this obsessive distress, individuals may develop increased attention to bodily sensations, misinterpretation of health-related stimuli, and excessive engagement in health-related behaviors (32). In this context, it is assumed that when an individual attempt to control or resist unexpected bodily sensations, health-related frightening thoughts, and anxiety feelings, the vigilance required for such control paradoxically re-establishes a connection with the very negative experiences they are trying to avoid. The final outcome is a vicious cycle (33). Therefore, hypervigilance toward bodily symptoms may intensify an individual’s health anxiety. It may also act as a mediating factor in the relationship between health anxiety and illness perception, thereby exacerbating the deterioration of conditions in older adults. Research suggests that heightened bodily awareness, or the extent to which individuals attend to and perceive bodily sensations, may represent an important vulnerability factor for the development and maintenance of anxiety and depressive symptoms, and may also contribute to psychosomatic disorders (34-35). Findings indicate that bodily vigilance increases among individuals with depressive and anxiety disorders, as they tend to excessively focus on potentially threatening bodily cues (35, 36). Increased awareness of possible changes in bodily sensations enhances the likelihood of perceiving physiological signals as threatening, which may contribute to heightened fear and bodily arousal (37). Research further shows that individuals with high levels of anxiety also demonstrate elevated levels of vigilance (38). A review of studies on illness perception, health anxiety, and bodily vigilance indicates that most research has focused on their relationship with panic disorder (39), anxiety disorders (40), or multiple sclerosis (41), among others. However, these variables have been relatively neglected in older adult populations, despite the fact that older adults—due to their heightened sensitivities—may be more vulnerable to health anxiety and increased vigilance toward illness and bodily symptoms. It is evident that individuals in this age group are more engaged with illness and physical symptoms than any other group. Therefore, the present study aims to examine the relationship between health anxiety and illness perception in older adults, with bodily vigilance as a mediating variable.
Methods
Study design
This study is basic research in terms of its objective and employs a descriptive–correlational design using structural equation modeling (SEM).
Participants
The target population consisted of elderly individuals attending medical clinics in the city of Urmia in 2024. Due to the absence of an accurate registry or statistical record regarding the number of elderly individuals attending medical clinics in Urmia, a convenience sampling method was employed. Accordingly, participants were recruited from individuals who were willing to participate in the study across 12 centers, including four public clinics, four private clinics, and four psychological clinics. The sample size was determined based on Kline (42) guideline, a widely used approach in SEM studies. According to Kline’s guideline, the recommended sample size for structural equation modeling ranges from 10 to 20 participants per estimated parameter, resulting in an estimated sample size of approximately 200 to 400 participants for the present model. Although the upper bound of this range was not achieved due to practical constraints, the final sample size of 200 participants meets the minimum recommended threshold and is considered adequate for PLS-SEM analysis. Previous methodological research has indicated that PLS-SEM is suitable for studies with relatively smaller sample sizes and complex models, particularly when the primary objective is prediction and theory development (47). In addition, given the observed effect sizes and significant path coefficients, the statistical power of the model can be considered acceptable. However, future studies with larger sample sizes are recommended to further enhance the robustness of the findings (47). Participants were not selected based on any specific clinical diagnosis of health anxiety; rather, the study aimed to assess varying levels of health anxiety within a general elderly clinical population.
Inclusion and exclusion criteria
Participants were included if they: provided informed consent; were aged 60 years or older; had the willingness and ability to participate voluntarily; possessed literacy skills to understand questionnaires; and had attended medical clinics in Urmia within the past six months; and obtained permission from their physician. Exclusion criteria included loss of willingness to cooperate at any stage and incorrect or incomplete responses to questionnaires, leading to data removal.
Following approval of the research proposal by the ethics committee and obtaining the necessary permissions, the research instruments were prepared, and the necessary coordination with medical clinics in Urmia was carried out. To reduce potential bias, the researcher was trained in standardized questionnaire administration procedures prior to data collection and analysis. Prior to data collection, the researcher was trained in standardized questionnaire administration procedures to ensure consistency across all interviews. Eligible participants (aged 60 years and above, willing to participate, and possessing basic literacy skills) were identified. After obtaining informed consent, the questionnaires were administered and collected in person. Given the older age groups of the participants and the possibility of limited literacy among some individuals, the questionnaires were administered through structured interviews conducted by the researcher. To minimize interviewer bias, the researcher followed a standardized protocol and read each item verbatim without interpretation or guidance. Participants’ responses were recorded exactly as expressed. In addition, efforts were made to ensure privacy and confidentiality during data collection in order to reduce social desirability bias.
Instruments
Health Anxiety Inventory
The Health Anxiety Inventory was used to assess health anxiety. The short form of this instrument was developed by Salkovskis and Warwick (25) and consists of 18 items. Each item includes four response options, each representing a declarative statement describing different aspects of health and illness. Respondents are required to select the statement that best describes their condition. The questionnaire comprises three main components: perceived likelihood of illness, negative consequences of illness, and general health concerns. The perceived likelihood of illness component is assessed by items 5, 6, 8, 9, 11, and 12. The negative consequences component includes items 13, 15, 16, 17, and 18. General health concerns are measured by items 1, 2, 3, 4, 7, 10, and 14. Scoring is based on a 4-point scale ranging from 0 to 3 for each item, where option A is scored 0, option B 1, option C 2, and option D 3. Regarding psychometric properties, the original version demonstrated good reliability, with test–retest reliability reported at 0.90 and Cronbach’s alpha ranging from 0.70 to 0.82. Validity was supported by a correlation of 0.63 with the Illness Attitudes Scale (IAS) (25), while Abramowitz et al., (43) reported a higher validity coefficient of 0.94. In the Iranian version, the questionnaire showed satisfactory internal consistency with a Cronbach’s alpha of 0.87, indicating acceptable reliability in the local population (44).
Illness Perception Questionnaire
The Brief Illness Perception Questionnaire was developed by Broadbent et al., (45) to assess cognitive and emotional representations of illness. It includes 9 items measuring consequences, timeline, personal control, treatment control, identity, concern, illness understanding, emotional response, and causes. The first eight items are rated on an 11-point scale (0–10), while the ninth is an open-ended question about perceived causes. The total score is calculated by summing or averaging the eight scored items, ranging from 0 to 80, with higher scores indicating more negative illness perceptions. Interpretation is typically: 0–20 low, 20–60 moderate, and above 60 high illness perception. The original version showed good reliability, with Cronbach’s alpha of 0.80 and test–retest reliability between 0.42 and 0.75, along with acceptable construct validity across different patient groups. The Persian version validated, demonstrated good internal consistency (α = 0.87) and acceptable content and concurrent validity based on expert review and correlations with related constructs (r = 0.32–0.63) (46).
Body Vigilance Scale
The Body Vigilance Scale was developed by Smith et al., (34) to assess the degree of attentional focus on internal bodily sensations. This scale consists of four items. The first three items assess the extent to which individuals attend to bodily sensations, their sensitivity to such sensations, and the amount of time they spend each day focusing on bodily processes. The fourth item assesses the extent to which individuals attend to 15 specific bodily sensations, each rated on a 0–10 scale. Therefore, the total score ranges from 0 to 180. These sensations represent common somatic symptoms characteristic of panic attacks. Smith et al., (34) confirmed the construct validity of the scale and reported a correlation of 0.68 with the Anxiety Sensitivity Questionnaire. They also reported a Cronbach’s alpha coefficient of 0.98 for the scale, indicating excellent internal consistency. Since no validated Persian version of the Body Vigilance Scale was available for the target population, the instrument was translated into Persian using a forward–backward translation procedure. In addition, face validity and content validity were qualitatively assessed by a panel of experts in psychology and health psychology to ensure cultural and conceptual equivalence for the elderly population. Minor linguistic adjustments were made based on expert feedback to improve clarity. The Persian version of the Body Vigilance Scale demonstrated satisfactory face, content, and construct validity, as confirmed by university professors and experts. The instrument also showed excellent reliability, with a Cronbach’s alpha of 0.96 and composite reliability (CR) of 0.964, along with adequate convergent validity (AVE = 0.78). Discriminant validity was also confirmed based on the HTMT criterion, with all values below 0.85, indicating strong psychometric validity of the scale. These analyses were conducted using SmartPLS software.
Statistical analysis
Three standardized questionnaires were administered in person at medical clinics in Urmia for data collection. To ensure accurate comprehension of the items, additional explanations were provided to participants when necessary. Descriptive statistical methods, including frequency, percentage, mean, standard deviation, and standard error, were used to summarize the data. Out of the initial 200 distributed questionnaires, all responses were complete and eligible for analysis; therefore, no cases were excluded due to missing data. No participant withdrew from the study after providing informed consent. In the inferential statistics section, the Pearson correlation coefficient and
Partial Least Squares Structural Equation Modeling (PLS-SEM) were applied to test the research hypotheses. Statistical analyses were conducted using SPSS and SmartPLS software.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Islamic Azad University, Urmia Branch (protocol code: IR.IAU.URIMA.REC.1403.003). All participants provided written informed consent prior to participation.
Results
Demographic characteristics
The descriptive statistics of the participants’ demographic characteristics, including education level, marital status, gender, and age, are presented in Table 1. As shown in Table 1, the majority of participants had a diploma or lower level of education (70%) and were married (92.5%). The mean age of the participants was 76.80 years (SD = 6.46), indicating that the sample primarily consisted of older adults in advanced age. Other demographic characteristics are reported in Table 1. The mean age of participants was 76.80 years (SD = 6.46), reflecting that the sample predominantly consisted of older adults in advanced stages of aging. Overall, the demographic profile suggests that the sample was largely composed of married elderly individuals with relatively low educational attainment.
The descriptive statistics for the study variables indicated that the mean score of health anxiety was 38.33 (SD = 11.54), the mean score of bodily vigilance was 99.29 (SD = 42.21), and the mean score of illness perception was 42.46 (SD = 18.50). The skewness and kurtosis values for all study variables (health anxiety, bodily vigilance, and illness perception) were within the acceptable range of ±2, suggesting no severe deviation from normal distribution. Overall, the findings indicate that the study variables approximately follow a normal distribution. A more detailed assessment of the normality assumptions is provided in the subsequent section.
Prior to conducting structural equation modeling, assumptions of normality, multicollinearity, and outliers were examined. Normality was assessed using skewness and kurtosis indices, as well as the Kolmogorov–Smirnov test. The results indicated that all study variables fell within acceptable ranges of skewness and kurtosis (± 2) and showed non-significant Kolmogorov–Smirnov statistics (p > 0.05), suggesting no serious deviation from normal distribution.
Outlier analysis was performed through standardized score inspection, and no extreme outliers were identified that could influence the results.
Multicollinearity was evaluated using tolerance and variance inflation factor (VIF) values at both measurement and structural levels. The results showed that tolerance values were above 0.10 and VIF values were below the critical threshold of 10, indicating no multicollinearity issues among the variables.
The correlation coefficients among the study variables are presented in Table 2. As illustrated, all variables demonstrate statistically significant positive correlations with each other at the 0.01 significance level. These findings indicate that health anxiety, bodily vigilance, and illness perception are significantly and positively interrelated. Accordingly, it can be concluded that the variables included in the model are meaningfully associated with one another, and the use of SEM is appropriate and justified. Although the correlation between bodily vigilance and illness perception was relatively high (r = 0.713), additional collinearity diagnostics indicated that all values were below the recommended threshold, confirming that multicollinearity was not a concern in the present model.
In the assessment of the measurement model, reliability was examined using Cronbach’s alpha, composite reliability (CR), and rho coefficient. The results are presented in Table 3. The findings indicate that all reliability indices for the study variables are within acceptable ranges. Cronbach’s alpha values exceeded the recommended threshold of 0.70 for all constructs, indicating satisfactory internal consistency. Similarly, rho coefficients were also above 0.70, confirming adequate reliability across all variables. In addition, CR values were higher than 0.70 for all constructs, further supporting the reliability of the measurement model. Convergent validity was confirmed as all constructs demonstrated Average Variance Extracted (AVE) values above the recommended threshold of 0.50, indicating that the constructs adequately explained more than half of the variance in their indicators. In addition, discriminant validity was assessed using the Heterotrait–Monotrait (HTMT) ratio, and all values were below the conservative threshold of 0.85, indicating satisfactory discriminant validity among the constructs.
In the assessment of the structural model, model fit indices were examined to evaluate the overall goodness-of-fit. The results of the model fit indices are presented in Table 4, and the path coefficients are illustrated in Figure 1. The results indicate that the Standardized Root Mean Square Residual (SRMR) value was 0.089, which reflects an acceptable level of model fit, as values closer to zero indicate better fit between the model and the data. The squared Euclidean distance (d_ULS) was 7.79, suggesting a small discrepancy between the estimated and saturated models. Similarly, the geodesic distance (d_G) was 4.22, indicating a satisfactory level of model fit. The Chi-square statistic was 5362.61, which is commonly used to assess overall model fit, where lower values indicate better model performance; however, this index is sensitive to sample size. Finally, the Normed Fit Index (NFI) was 0.891, which is slightly below the recommended threshold of 0.90 but still close to the acceptable range, indicating an acceptable but not optimal level of model fit. Overall, the findings suggest that the structural model demonstrates an acceptable level of fit across most indices, with the NFI being slightly below the ideal cutoff. Overall, the model fit indices indicated an acceptable but not optimal model fit. Specifically, SRMR was slightly above the recommended threshold, and NFI was marginally below the ideal cut-off value. Therefore, these indices should be interpreted with caution.
Research shows that illness perception influences individuals’ self-care behaviors (16, 17). Studies have demonstrated that illness perception is one of the most important predictors of low-level adaptation outcomes, including social dysfunction, fatigue, anxiety, depression, and self-esteem (18). Furthermore, research indicates that illness perception has an impact on individuals’ mental health and psychological quality of life (19). In addition, a study found a significant relationship between illness perception, quality of life, and optimism in patients (20). One of the issues that older adults—especially those who are aware of having a disease or are concerned about becoming ill—struggle with is health anxiety (21). This is because older adults, due to aging and reduced immune function, often experience numerous thoughts and concerns about their health (22).
Health anxiety, or illness anxiety disorder, was first introduced in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM) 5 under the category of somatic symptom disorders. Previously, in DSM-III and DSM-IV, it was referred to as hypochondriasis (23). This disorder creates a chronic, episodic, and recurrent condition that often begins in early adulthood and worsens with age, affecting men and women equally. Health anxiety refers to a condition characterized by the misinterpretation of bodily sensations or physical changes as signs of a serious illness. Individuals affected by health anxiety are preoccupied with the belief that they are currently suffering from a physical disease (24). Evidence suggests that health anxiety has a dimensional structure, ranging from the absence of concern about one’s health at one end to excessive anxiety about health at the other (25). Health anxiety differs from general anxiety because it involves irrational concerns that physical symptoms indicate the presence of a serious illness (21, 26). Salkovskis and Warwick (27) described four dysfunctional health-related beliefs that are particularly important for understanding health anxiety: the likelihood of having or developing a serious illness, fear of illness, perceived inability to cope with illness, and the belief that medical services are insufficient for effective treatment.
In its severe form, health anxiety has a significant long-term impact on individuals’ self-rated physical and mental health functioning, as well as on healthcare costs (28). In this disorder, physical symptoms may be absent or very mild; therefore, the individual’s distress is not primarily caused by somatic symptoms, but rather by anxiety and worry about the causes and consequences of an undiagnosed illness (29-31). As a result of this obsessive distress, individuals may develop increased attention to bodily sensations, misinterpretation of health-related stimuli, and excessive engagement in health-related behaviors (32). In this context, it is assumed that when an individual attempt to control or resist unexpected bodily sensations, health-related frightening thoughts, and anxiety feelings, the vigilance required for such control paradoxically re-establishes a connection with the very negative experiences they are trying to avoid. The final outcome is a vicious cycle (33). Therefore, hypervigilance toward bodily symptoms may intensify an individual’s health anxiety. It may also act as a mediating factor in the relationship between health anxiety and illness perception, thereby exacerbating the deterioration of conditions in older adults. Research suggests that heightened bodily awareness, or the extent to which individuals attend to and perceive bodily sensations, may represent an important vulnerability factor for the development and maintenance of anxiety and depressive symptoms, and may also contribute to psychosomatic disorders (34-35). Findings indicate that bodily vigilance increases among individuals with depressive and anxiety disorders, as they tend to excessively focus on potentially threatening bodily cues (35, 36). Increased awareness of possible changes in bodily sensations enhances the likelihood of perceiving physiological signals as threatening, which may contribute to heightened fear and bodily arousal (37). Research further shows that individuals with high levels of anxiety also demonstrate elevated levels of vigilance (38). A review of studies on illness perception, health anxiety, and bodily vigilance indicates that most research has focused on their relationship with panic disorder (39), anxiety disorders (40), or multiple sclerosis (41), among others. However, these variables have been relatively neglected in older adult populations, despite the fact that older adults—due to their heightened sensitivities—may be more vulnerable to health anxiety and increased vigilance toward illness and bodily symptoms. It is evident that individuals in this age group are more engaged with illness and physical symptoms than any other group. Therefore, the present study aims to examine the relationship between health anxiety and illness perception in older adults, with bodily vigilance as a mediating variable.
Methods
Study design
This study is basic research in terms of its objective and employs a descriptive–correlational design using structural equation modeling (SEM).
Participants
The target population consisted of elderly individuals attending medical clinics in the city of Urmia in 2024. Due to the absence of an accurate registry or statistical record regarding the number of elderly individuals attending medical clinics in Urmia, a convenience sampling method was employed. Accordingly, participants were recruited from individuals who were willing to participate in the study across 12 centers, including four public clinics, four private clinics, and four psychological clinics. The sample size was determined based on Kline (42) guideline, a widely used approach in SEM studies. According to Kline’s guideline, the recommended sample size for structural equation modeling ranges from 10 to 20 participants per estimated parameter, resulting in an estimated sample size of approximately 200 to 400 participants for the present model. Although the upper bound of this range was not achieved due to practical constraints, the final sample size of 200 participants meets the minimum recommended threshold and is considered adequate for PLS-SEM analysis. Previous methodological research has indicated that PLS-SEM is suitable for studies with relatively smaller sample sizes and complex models, particularly when the primary objective is prediction and theory development (47). In addition, given the observed effect sizes and significant path coefficients, the statistical power of the model can be considered acceptable. However, future studies with larger sample sizes are recommended to further enhance the robustness of the findings (47). Participants were not selected based on any specific clinical diagnosis of health anxiety; rather, the study aimed to assess varying levels of health anxiety within a general elderly clinical population.
Inclusion and exclusion criteria
Participants were included if they: provided informed consent; were aged 60 years or older; had the willingness and ability to participate voluntarily; possessed literacy skills to understand questionnaires; and had attended medical clinics in Urmia within the past six months; and obtained permission from their physician. Exclusion criteria included loss of willingness to cooperate at any stage and incorrect or incomplete responses to questionnaires, leading to data removal.
Following approval of the research proposal by the ethics committee and obtaining the necessary permissions, the research instruments were prepared, and the necessary coordination with medical clinics in Urmia was carried out. To reduce potential bias, the researcher was trained in standardized questionnaire administration procedures prior to data collection and analysis. Prior to data collection, the researcher was trained in standardized questionnaire administration procedures to ensure consistency across all interviews. Eligible participants (aged 60 years and above, willing to participate, and possessing basic literacy skills) were identified. After obtaining informed consent, the questionnaires were administered and collected in person. Given the older age groups of the participants and the possibility of limited literacy among some individuals, the questionnaires were administered through structured interviews conducted by the researcher. To minimize interviewer bias, the researcher followed a standardized protocol and read each item verbatim without interpretation or guidance. Participants’ responses were recorded exactly as expressed. In addition, efforts were made to ensure privacy and confidentiality during data collection in order to reduce social desirability bias.
Instruments
Health Anxiety Inventory
The Health Anxiety Inventory was used to assess health anxiety. The short form of this instrument was developed by Salkovskis and Warwick (25) and consists of 18 items. Each item includes four response options, each representing a declarative statement describing different aspects of health and illness. Respondents are required to select the statement that best describes their condition. The questionnaire comprises three main components: perceived likelihood of illness, negative consequences of illness, and general health concerns. The perceived likelihood of illness component is assessed by items 5, 6, 8, 9, 11, and 12. The negative consequences component includes items 13, 15, 16, 17, and 18. General health concerns are measured by items 1, 2, 3, 4, 7, 10, and 14. Scoring is based on a 4-point scale ranging from 0 to 3 for each item, where option A is scored 0, option B 1, option C 2, and option D 3. Regarding psychometric properties, the original version demonstrated good reliability, with test–retest reliability reported at 0.90 and Cronbach’s alpha ranging from 0.70 to 0.82. Validity was supported by a correlation of 0.63 with the Illness Attitudes Scale (IAS) (25), while Abramowitz et al., (43) reported a higher validity coefficient of 0.94. In the Iranian version, the questionnaire showed satisfactory internal consistency with a Cronbach’s alpha of 0.87, indicating acceptable reliability in the local population (44).
Illness Perception Questionnaire
The Brief Illness Perception Questionnaire was developed by Broadbent et al., (45) to assess cognitive and emotional representations of illness. It includes 9 items measuring consequences, timeline, personal control, treatment control, identity, concern, illness understanding, emotional response, and causes. The first eight items are rated on an 11-point scale (0–10), while the ninth is an open-ended question about perceived causes. The total score is calculated by summing or averaging the eight scored items, ranging from 0 to 80, with higher scores indicating more negative illness perceptions. Interpretation is typically: 0–20 low, 20–60 moderate, and above 60 high illness perception. The original version showed good reliability, with Cronbach’s alpha of 0.80 and test–retest reliability between 0.42 and 0.75, along with acceptable construct validity across different patient groups. The Persian version validated, demonstrated good internal consistency (α = 0.87) and acceptable content and concurrent validity based on expert review and correlations with related constructs (r = 0.32–0.63) (46).
Body Vigilance Scale
The Body Vigilance Scale was developed by Smith et al., (34) to assess the degree of attentional focus on internal bodily sensations. This scale consists of four items. The first three items assess the extent to which individuals attend to bodily sensations, their sensitivity to such sensations, and the amount of time they spend each day focusing on bodily processes. The fourth item assesses the extent to which individuals attend to 15 specific bodily sensations, each rated on a 0–10 scale. Therefore, the total score ranges from 0 to 180. These sensations represent common somatic symptoms characteristic of panic attacks. Smith et al., (34) confirmed the construct validity of the scale and reported a correlation of 0.68 with the Anxiety Sensitivity Questionnaire. They also reported a Cronbach’s alpha coefficient of 0.98 for the scale, indicating excellent internal consistency. Since no validated Persian version of the Body Vigilance Scale was available for the target population, the instrument was translated into Persian using a forward–backward translation procedure. In addition, face validity and content validity were qualitatively assessed by a panel of experts in psychology and health psychology to ensure cultural and conceptual equivalence for the elderly population. Minor linguistic adjustments were made based on expert feedback to improve clarity. The Persian version of the Body Vigilance Scale demonstrated satisfactory face, content, and construct validity, as confirmed by university professors and experts. The instrument also showed excellent reliability, with a Cronbach’s alpha of 0.96 and composite reliability (CR) of 0.964, along with adequate convergent validity (AVE = 0.78). Discriminant validity was also confirmed based on the HTMT criterion, with all values below 0.85, indicating strong psychometric validity of the scale. These analyses were conducted using SmartPLS software.
Statistical analysis
Three standardized questionnaires were administered in person at medical clinics in Urmia for data collection. To ensure accurate comprehension of the items, additional explanations were provided to participants when necessary. Descriptive statistical methods, including frequency, percentage, mean, standard deviation, and standard error, were used to summarize the data. Out of the initial 200 distributed questionnaires, all responses were complete and eligible for analysis; therefore, no cases were excluded due to missing data. No participant withdrew from the study after providing informed consent. In the inferential statistics section, the Pearson correlation coefficient and
Partial Least Squares Structural Equation Modeling (PLS-SEM) were applied to test the research hypotheses. Statistical analyses were conducted using SPSS and SmartPLS software.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Islamic Azad University, Urmia Branch (protocol code: IR.IAU.URIMA.REC.1403.003). All participants provided written informed consent prior to participation.
Results
Demographic characteristics
The descriptive statistics of the participants’ demographic characteristics, including education level, marital status, gender, and age, are presented in Table 1. As shown in Table 1, the majority of participants had a diploma or lower level of education (70%) and were married (92.5%). The mean age of the participants was 76.80 years (SD = 6.46), indicating that the sample primarily consisted of older adults in advanced age. Other demographic characteristics are reported in Table 1. The mean age of participants was 76.80 years (SD = 6.46), reflecting that the sample predominantly consisted of older adults in advanced stages of aging. Overall, the demographic profile suggests that the sample was largely composed of married elderly individuals with relatively low educational attainment.
The descriptive statistics for the study variables indicated that the mean score of health anxiety was 38.33 (SD = 11.54), the mean score of bodily vigilance was 99.29 (SD = 42.21), and the mean score of illness perception was 42.46 (SD = 18.50). The skewness and kurtosis values for all study variables (health anxiety, bodily vigilance, and illness perception) were within the acceptable range of ±2, suggesting no severe deviation from normal distribution. Overall, the findings indicate that the study variables approximately follow a normal distribution. A more detailed assessment of the normality assumptions is provided in the subsequent section.
Prior to conducting structural equation modeling, assumptions of normality, multicollinearity, and outliers were examined. Normality was assessed using skewness and kurtosis indices, as well as the Kolmogorov–Smirnov test. The results indicated that all study variables fell within acceptable ranges of skewness and kurtosis (± 2) and showed non-significant Kolmogorov–Smirnov statistics (p > 0.05), suggesting no serious deviation from normal distribution.
Outlier analysis was performed through standardized score inspection, and no extreme outliers were identified that could influence the results.
Multicollinearity was evaluated using tolerance and variance inflation factor (VIF) values at both measurement and structural levels. The results showed that tolerance values were above 0.10 and VIF values were below the critical threshold of 10, indicating no multicollinearity issues among the variables.
The correlation coefficients among the study variables are presented in Table 2. As illustrated, all variables demonstrate statistically significant positive correlations with each other at the 0.01 significance level. These findings indicate that health anxiety, bodily vigilance, and illness perception are significantly and positively interrelated. Accordingly, it can be concluded that the variables included in the model are meaningfully associated with one another, and the use of SEM is appropriate and justified. Although the correlation between bodily vigilance and illness perception was relatively high (r = 0.713), additional collinearity diagnostics indicated that all values were below the recommended threshold, confirming that multicollinearity was not a concern in the present model.
In the assessment of the measurement model, reliability was examined using Cronbach’s alpha, composite reliability (CR), and rho coefficient. The results are presented in Table 3. The findings indicate that all reliability indices for the study variables are within acceptable ranges. Cronbach’s alpha values exceeded the recommended threshold of 0.70 for all constructs, indicating satisfactory internal consistency. Similarly, rho coefficients were also above 0.70, confirming adequate reliability across all variables. In addition, CR values were higher than 0.70 for all constructs, further supporting the reliability of the measurement model. Convergent validity was confirmed as all constructs demonstrated Average Variance Extracted (AVE) values above the recommended threshold of 0.50, indicating that the constructs adequately explained more than half of the variance in their indicators. In addition, discriminant validity was assessed using the Heterotrait–Monotrait (HTMT) ratio, and all values were below the conservative threshold of 0.85, indicating satisfactory discriminant validity among the constructs.
In the assessment of the structural model, model fit indices were examined to evaluate the overall goodness-of-fit. The results of the model fit indices are presented in Table 4, and the path coefficients are illustrated in Figure 1. The results indicate that the Standardized Root Mean Square Residual (SRMR) value was 0.089, which reflects an acceptable level of model fit, as values closer to zero indicate better fit between the model and the data. The squared Euclidean distance (d_ULS) was 7.79, suggesting a small discrepancy between the estimated and saturated models. Similarly, the geodesic distance (d_G) was 4.22, indicating a satisfactory level of model fit. The Chi-square statistic was 5362.61, which is commonly used to assess overall model fit, where lower values indicate better model performance; however, this index is sensitive to sample size. Finally, the Normed Fit Index (NFI) was 0.891, which is slightly below the recommended threshold of 0.90 but still close to the acceptable range, indicating an acceptable but not optimal level of model fit. Overall, the findings suggest that the structural model demonstrates an acceptable level of fit across most indices, with the NFI being slightly below the ideal cutoff. Overall, the model fit indices indicated an acceptable but not optimal model fit. Specifically, SRMR was slightly above the recommended threshold, and NFI was marginally below the ideal cut-off value. Therefore, these indices should be interpreted with caution.
Table 1. Demographic characteristics of the participants and descriptive statistics of age
| Variable | Categories | Frequency | Percentage |
| Education | Diploma or lower | 140 | 70% |
| Associate degree / Bachelor’s degree | 39 | 19.5% | |
| Master’s degree and higher | 21 | 10.5% | |
| Marital status | Married | 185 | 92.5% |
| Single | 15 | 7.5% | |
| Gender | Male | 110 | 55% |
| Female | 90 | 45% | |
| Age | 200 (Mean ± SD) | 76.80 | 6.46 |
Table 2. Correlation matrix of study variables
| Variables | 1 | 2 | 3 |
| 1. Health anxiety | — | ||
| 2. Bodily vigilance | 0.305** | — | |
| 3. Illness perception | 0.497** | 0.713** | — |
Table 3. Measurement model fit indices (Reliability indicators)
| Variables | Cronbach’s Alpha | Rho | Composite reliability (CR) | AVE |
| Health anxiety | 0.922 | 0.926 | 0.931 | 0.72 |
| Bodily vigilance | 0.960 | 0.943 | 0.964 | 0.78 |
| Illness perception | 0.920 | 0.964 | 0.935 | 0.70 |
Figure 1. Structural equation model of the relationships among health anxiety, bodily symptom vigilance, and illness perception
Table 4. Structural model fit indices
The results of structural equation modeling revealed that all proposed hypotheses were statistically significant and supported by the data. Specifically, health anxiety demonstrated a positive and significant direct effect on illness perception (β = 0.313, t = 5.04, p < 0.001), indicating that higher levels of health anxiety are associated with stronger perceptions of illness among elderly individuals. Furthermore, bodily vigilance showed a strong and significant positive effect on illness perception (β = 0.620, t = 10.60, p < 0.001), suggesting that increased attention to bodily sensations substantially enhances illness perception. In addition, health anxiety had a significant positive effect on bodily vigilance (β = 0.323, t = 5.27, p < 0.001), confirming that individuals with higher health anxiety exhibit greater monitoring of bodily symptoms. Most importantly, the mediating role of bodily vigilance in the relationship between health anxiety and illness perception was also confirmed (β = 0.200, t = 4.26, p < 0.001). The indirect effect was also supported by bootstrapped confidence intervals, which did not include zero, confirming the significance of the mediation effect. The coefficient of determination (R²) indicated that health anxiety and bodily vigilance explained a substantial proportion of variance in illness perception (R² = 0.56), reflecting moderate explanatory power. In addition, R² for bodily vigilance was 0.42, indicating moderate predictive accuracy of the model. Effect size (f²) values showed that health anxiety had a medium effect on bodily vigilance (f² = 0.18), while bodily vigilance had a large effect on illness perception (f² = 0.42), and health anxiety had a small-to-medium effect on illness perception (f² = 0.12). Overall, the results provide strong empirical support for all four hypotheses of the study and confirm the robustness of the proposed structural model.
| Index | Value | Evaluation |
| SRMR | 0.089 | Acceptable |
| d_ULS | 7.79 | Acceptable |
| d_G | 4.22 | Acceptable |
| Chi-Square | 5362.61 | Acceptable |
| NFI | 0.891 | Near acceptable |
The results of structural equation modeling revealed that all proposed hypotheses were statistically significant and supported by the data. Specifically, health anxiety demonstrated a positive and significant direct effect on illness perception (β = 0.313, t = 5.04, p < 0.001), indicating that higher levels of health anxiety are associated with stronger perceptions of illness among elderly individuals. Furthermore, bodily vigilance showed a strong and significant positive effect on illness perception (β = 0.620, t = 10.60, p < 0.001), suggesting that increased attention to bodily sensations substantially enhances illness perception. In addition, health anxiety had a significant positive effect on bodily vigilance (β = 0.323, t = 5.27, p < 0.001), confirming that individuals with higher health anxiety exhibit greater monitoring of bodily symptoms. Most importantly, the mediating role of bodily vigilance in the relationship between health anxiety and illness perception was also confirmed (β = 0.200, t = 4.26, p < 0.001). The indirect effect was also supported by bootstrapped confidence intervals, which did not include zero, confirming the significance of the mediation effect. The coefficient of determination (R²) indicated that health anxiety and bodily vigilance explained a substantial proportion of variance in illness perception (R² = 0.56), reflecting moderate explanatory power. In addition, R² for bodily vigilance was 0.42, indicating moderate predictive accuracy of the model. Effect size (f²) values showed that health anxiety had a medium effect on bodily vigilance (f² = 0.18), while bodily vigilance had a large effect on illness perception (f² = 0.42), and health anxiety had a small-to-medium effect on illness perception (f² = 0.12). Overall, the results provide strong empirical support for all four hypotheses of the study and confirm the robustness of the proposed structural model.
Table 5. Structural path coefficients for direct and indirect effects (hypotheses testing)
| Hypothesis path | Path coefficient (β) | Standard deviation | t-value | p | Result |
| Health anxiety → Illness perception | 0.313 | 0.062 | 5.04 | 0.001 | Supported |
| Bodily vigilance → Illness perception | 0.620 | 0.058 | 10.60 | 0.001 | Supported |
| Health anxiety → Bodily vigilance | 0.323 | 0.061 | 5.27 | 0.001 | Supported |
| Health anxiety → Bodily vigilance → Illness perception (Indirect effect) | 0.200 | 0.047 | 4.26 | 0.001 | Supported |
Discussion
This study aimed to examine the role of health anxiety in predicting illness perception among older adults. Accordingly, the first hypothesis proposed that health anxiety is associated with illness perception in elderly individuals. The findings of the present study indicated that health anxiety has a positive and significant relationship with illness perception, meaning that higher levels of health anxiety are associated with more negative and exaggerated perceptions of illness among older adults. This result suggests that elderly individuals with higher anxiety levels are more likely to interpret bodily sensations as threatening and to experience excessive concerns regarding their health status.
The findings of the present study revealed that health anxiety has a significant positive relationship with illness perception in older adults. This result is consistent with the theoretical assumptions of Leventhal’s self-regulation model (13), which emphasizes that individuals construct cognitive representations of illness based on perceived bodily cues, emotional responses, and health-related beliefs. In line with this framework, older adults with higher levels of health anxiety are more likely to interpret bodily sensations as indicators of serious disease, thereby forming more threatening and maladaptive illness representations. This finding is supported by prior empirical research indicating that health anxiety is closely associated with distorted interpretations of bodily sensations and exaggerated illness-related beliefs. For example, Fergusson-White (10) and Gåfvels and Wändell (11) emphasized that illness perception is shaped by cognitive representations such as symptom identity, perceived consequences, and controllability. Individuals with elevated health anxiety tend to negatively bias these cognitive dimensions, particularly by overestimating the severity and consequences of symptoms. Similarly, Salkovskis and Warwick (27) highlighted that dysfunctional beliefs about the likelihood of illness and the perceived inability to cope with disease are central mechanisms underlying health anxiety, which directly contribute to intensified illness perceptions. From a developmental perspective, this relationship may be particularly pronounced in older adults. As highlighted in the literature, aging is associated with increased physical vulnerability, reduced immune function, and a higher frequency of somatic experiences (8, 22). These age-related changes create a context in which health-related concerns are more easily activated and maintained. Consequently, older adults with heightened health anxiety may be more prone to misinterpret normal bodily changes as pathological, thereby reinforcing maladaptive illness perceptions (7). Furthermore, consistent with cognitive-behavioral accounts of health anxiety, individuals with elevated anxiety demonstrate increased attention to bodily sensations and a tendency toward catastrophic interpretation of ambiguous physical cues (25, 32). This hypervigilance not only intensifies emotional distress but also strengthens maladaptive cognitive schemas regarding illness identity, chronicity, and consequences. In this regard, the findings of the present study align with previous evidence showing that heightened health anxiety is associated with increased perceived vulnerability to disease and exaggerated interpretation of somatic symptoms (26, 30). Additionally, this result can be understood in the context of the cyclical interaction between cognition, emotion, and bodily monitoring. As individuals become increasingly preoccupied with health-related concerns, they engage in excessive monitoring of bodily sensations, which paradoxically reinforces their perception of illness and strengthens anxiety-related interpretations (33). This feedback loop ultimately leads to a more negative and rigid illness perception, particularly in vulnerable populations such as older adults.
The second hypothesis of the present study proposed that bodily vigilance positively predicts illness perception in older adults. The findings confirmed this hypothesis, indicating that increased attentional focus on bodily sensations is significantly associated with more negative and intensified illness perceptions among elderly individuals. In other words, older adults who are more engaged in monitoring their internal bodily states are more likely to interpret normal physiological changes as signs of illness, which contributes to a heightened sense of vulnerability and a more threatening view of their health status. This finding can be understood in light of the conceptualization of illness perception as a cognitive representation of one’s health condition, which includes beliefs about symptoms, consequences, and controllability of disease (13). According to this framework, individuals construct their understanding of illness based on perceived bodily signals and the way they attend to and interpret these signals. Therefore, when attention is excessively directed toward bodily sensations, especially in a hypervigilant manner, the likelihood of misinterpreting benign or normal physical experiences as pathological increases. In older adults, this process may be particularly salient. Aging is associated with a wide range of biological and physiological changes, which naturally increase the frequency of bodily sensations (8). These age-related changes can make bodily cues more noticeable and therefore more likely to be the focus of attention. As a result, elderly individuals who exhibit higher bodily vigilance may become more sensitive to these internal cues and more prone to interpreting them as indicators of serious illness. This heightened attentional focus can gradually shape a more negative cognitive representation of health, in which bodily sensations are seen as threatening rather than neutral or adaptive. From a psychological perspective, illness perception is not merely a reflection of physical condition, but rather a subjective and cognitively constructed process that is influenced by attention, interpretation, and personal beliefs (10). Within this context, bodily vigilance functions as a key cognitive mechanism that shapes how internal bodily information is processed. When individuals continuously monitor their bodily sensations, this sustained attention increases the salience of physical experiences, thereby reinforcing concerns about health and strengthening illness-related beliefs.
The third hypothesis proposed that health anxiety significantly predicts bodily vigilance in older adults. The findings of the present study supported this hypothesis, indicating that higher levels of health-related anxiety are associated with increased monitoring and heightened attentional focus on bodily sensations. In other words, older adults with elevated health anxiety are more likely to engage in persistent scanning of their internal bodily states and to allocate greater cognitive attention to somatic cues, even in the absence of objective medical evidence. This finding is consistent with the conceptual understanding of health anxiety as a condition characterized by the misinterpretation of bodily sensations or physical changes as signs of serious illness (24). Individuals affected by health anxiety are preoccupied with the belief that they may be suffering from a physical disease, which leads to sustained attention toward bodily signals and heightened sensitivity to internal changes. This cognitive orientation naturally facilitates increased bodily vigilance, as individuals continuously attempt to detect possible indicators of illness. In older adults, this relationship may be particularly pronounced. Aging is associated with numerous physiological changes and reduced immune functioning, which increase the frequency and salience of bodily sensations (8). These changes can intensify health-related concerns and provide a constant source of bodily cues that attract attention. As a result, individuals with higher levels of health anxiety may be more likely to interpret these normal age-related sensations as signs of serious illness, thereby reinforcing continuous monitoring of the body. From a cognitive perspective, health anxiety is also associated with dysfunctional health-related beliefs, including overestimation of the likelihood of illness, fear of illness, perceived inability to cope with disease, and doubts about the effectiveness of medical care (27). These maladaptive beliefs contribute to increased vigilance toward bodily sensations, as individuals attempt to achieve certainty about their health status. However, this heightened focus on the body does not reduce anxiety; rather, it maintains and intensifies it by increasing awareness of bodily sensations that may otherwise be ignored.
The fourth hypothesis proposed that bodily vigilance mediates the relationship between health anxiety and illness perception in older adults. The findings of the present study confirmed this hypothesis, indicating that bodily vigilance plays a significant mediating role in this relationship. In other words, health anxiety not only exerts a direct effect on illness perception, but also influences illness perception indirectly through increased attentional focus on bodily sensations. This suggests that older adults with higher levels of health anxiety are more likely to engage in excessive monitoring of their bodily states, which in turn contributes to more negative and intensified perceptions of illness. This finding can be understood within the conceptualization of health anxiety as a condition characterized by the misinterpretation of bodily sensations or physical changes as signs of serious illness (24). Individuals with health anxiety are preoccupied with the belief that they are suffering from a physical disease, which increases their attention to internal bodily cues. This heightened attentional focus constitutes bodily vigilance, which serves as a cognitive mechanism through which health anxiety is translated into illness perception. In line with Leventhal’s self-regulation model, illness perception is shaped by individuals’ cognitive representations of symptoms, perceived consequences, and controllability of illness (13). Accordingly, when bodily sensations are continuously monitored and selectively attended to, they are more likely to be incorporated into these cognitive representations. In older adults, this process may be particularly pronounced due to age-related physiological changes, increased frequency of somatic experiences, and reduced physical resilience (8). These conditions make bodily sensations more salient and more likely to be interpreted as indicators of illness.
Furthermore, health anxiety involves dysfunctional beliefs about the likelihood of illness, fear of disease, perceived inability to cope with illness, and doubts regarding medical reassurance (27). These maladaptive beliefs intensify attention toward bodily sensations and increase the tendency to interpret ambiguous physical cues as threatening. As a result, bodily vigilance becomes a central pathway through which cognitive and emotional concerns about health are transformed into illness-related interpretations. Within this framework, bodily vigilance acts as a mediating cognitive process that links emotional vulnerability (health anxiety) to cognitive outcomes (illness perception). As individuals increasingly monitor their internal bodily states, they become more likely to detect normal physiological sensations, which are then interpreted through the lens of health-related fears.
Conclusion
The findings indicated that health anxiety had a significant positive effect on both bodily vigilance and illness perception, and bodily vigilance also significantly predicted illness perception. In addition, bodily vigilance was confirmed as a significant mediator in the relationship between health anxiety and illness perception. These results suggest that illness perception in older adults is shaped through both direct emotional-cognitive processes and indirect attentional mechanisms. From a theoretical perspective, the findings support cognitive-behavioral models of health anxiety, emphasizing the role of maladaptive beliefs and attentional bias toward bodily sensations. Practically, the results highlight the importance of targeting both health anxiety and excessive body monitoring in psychological interventions for older adults.
Study limitations
This study had some limitations. The cross-sectional design limits causal interpretations, and the use of convenience sampling restricts generalizability. In addition, reliance on self-report measures may have introduced bias, and medical variables such as comorbidities were not controlled. In terms of practical implications, it is recommended that health professionals screen for health anxiety in the elderly populations and use interventions such as cognitive-behavioral therapy to reduce maladaptive health beliefs and bodily hypervigilance. Future research should employ longitudinal designs and broader samples to better clarify causal relationships among these variables. In addition, participants were recruited from clinical settings without formal diagnostic screening for health anxiety. Therefore, the sample may include individuals with varying levels of health anxiety rather than clinically diagnosed cases, which should be considered when interpreting the findings. Furthermore, due to the use of interviewer-administered questionnaires for some participants, the possibility of interviewer bias and social desirability bias cannot be completely ruled out. Although standardized administration procedures were applied to minimize these effects, future studies are recommended to use multiple trained interviewers and to assess inter-rater reliability. Another limitation of the present study is the absence of inter-rater reliability assessment, as data coding and analysis were conducted by a single researcher.
Conflict of interests
The authors declare no conflict if interests.
Acknowledgments
The authors sincerely appreciate the participation of all elderly individuals in this study.
Funding
None
Authors' contributions
S.M. Conceptualization, Data Curation, Formal Analysis, Investigation, Writing – Original Draft. E.G. Methodology, Validation, Writing – Review & Editing. K.B. Investigation, Resources, Literature Review, Writing – Review & Editing. M.G. Conceptualization, Supervision, Project Administration, Validation, Writing – Review & Editing. All authors read and approved the final manuscript and agreed to be accountable for all aspects of the work.
References
The findings of the present study revealed that health anxiety has a significant positive relationship with illness perception in older adults. This result is consistent with the theoretical assumptions of Leventhal’s self-regulation model (13), which emphasizes that individuals construct cognitive representations of illness based on perceived bodily cues, emotional responses, and health-related beliefs. In line with this framework, older adults with higher levels of health anxiety are more likely to interpret bodily sensations as indicators of serious disease, thereby forming more threatening and maladaptive illness representations. This finding is supported by prior empirical research indicating that health anxiety is closely associated with distorted interpretations of bodily sensations and exaggerated illness-related beliefs. For example, Fergusson-White (10) and Gåfvels and Wändell (11) emphasized that illness perception is shaped by cognitive representations such as symptom identity, perceived consequences, and controllability. Individuals with elevated health anxiety tend to negatively bias these cognitive dimensions, particularly by overestimating the severity and consequences of symptoms. Similarly, Salkovskis and Warwick (27) highlighted that dysfunctional beliefs about the likelihood of illness and the perceived inability to cope with disease are central mechanisms underlying health anxiety, which directly contribute to intensified illness perceptions. From a developmental perspective, this relationship may be particularly pronounced in older adults. As highlighted in the literature, aging is associated with increased physical vulnerability, reduced immune function, and a higher frequency of somatic experiences (8, 22). These age-related changes create a context in which health-related concerns are more easily activated and maintained. Consequently, older adults with heightened health anxiety may be more prone to misinterpret normal bodily changes as pathological, thereby reinforcing maladaptive illness perceptions (7). Furthermore, consistent with cognitive-behavioral accounts of health anxiety, individuals with elevated anxiety demonstrate increased attention to bodily sensations and a tendency toward catastrophic interpretation of ambiguous physical cues (25, 32). This hypervigilance not only intensifies emotional distress but also strengthens maladaptive cognitive schemas regarding illness identity, chronicity, and consequences. In this regard, the findings of the present study align with previous evidence showing that heightened health anxiety is associated with increased perceived vulnerability to disease and exaggerated interpretation of somatic symptoms (26, 30). Additionally, this result can be understood in the context of the cyclical interaction between cognition, emotion, and bodily monitoring. As individuals become increasingly preoccupied with health-related concerns, they engage in excessive monitoring of bodily sensations, which paradoxically reinforces their perception of illness and strengthens anxiety-related interpretations (33). This feedback loop ultimately leads to a more negative and rigid illness perception, particularly in vulnerable populations such as older adults.
The second hypothesis of the present study proposed that bodily vigilance positively predicts illness perception in older adults. The findings confirmed this hypothesis, indicating that increased attentional focus on bodily sensations is significantly associated with more negative and intensified illness perceptions among elderly individuals. In other words, older adults who are more engaged in monitoring their internal bodily states are more likely to interpret normal physiological changes as signs of illness, which contributes to a heightened sense of vulnerability and a more threatening view of their health status. This finding can be understood in light of the conceptualization of illness perception as a cognitive representation of one’s health condition, which includes beliefs about symptoms, consequences, and controllability of disease (13). According to this framework, individuals construct their understanding of illness based on perceived bodily signals and the way they attend to and interpret these signals. Therefore, when attention is excessively directed toward bodily sensations, especially in a hypervigilant manner, the likelihood of misinterpreting benign or normal physical experiences as pathological increases. In older adults, this process may be particularly salient. Aging is associated with a wide range of biological and physiological changes, which naturally increase the frequency of bodily sensations (8). These age-related changes can make bodily cues more noticeable and therefore more likely to be the focus of attention. As a result, elderly individuals who exhibit higher bodily vigilance may become more sensitive to these internal cues and more prone to interpreting them as indicators of serious illness. This heightened attentional focus can gradually shape a more negative cognitive representation of health, in which bodily sensations are seen as threatening rather than neutral or adaptive. From a psychological perspective, illness perception is not merely a reflection of physical condition, but rather a subjective and cognitively constructed process that is influenced by attention, interpretation, and personal beliefs (10). Within this context, bodily vigilance functions as a key cognitive mechanism that shapes how internal bodily information is processed. When individuals continuously monitor their bodily sensations, this sustained attention increases the salience of physical experiences, thereby reinforcing concerns about health and strengthening illness-related beliefs.
The third hypothesis proposed that health anxiety significantly predicts bodily vigilance in older adults. The findings of the present study supported this hypothesis, indicating that higher levels of health-related anxiety are associated with increased monitoring and heightened attentional focus on bodily sensations. In other words, older adults with elevated health anxiety are more likely to engage in persistent scanning of their internal bodily states and to allocate greater cognitive attention to somatic cues, even in the absence of objective medical evidence. This finding is consistent with the conceptual understanding of health anxiety as a condition characterized by the misinterpretation of bodily sensations or physical changes as signs of serious illness (24). Individuals affected by health anxiety are preoccupied with the belief that they may be suffering from a physical disease, which leads to sustained attention toward bodily signals and heightened sensitivity to internal changes. This cognitive orientation naturally facilitates increased bodily vigilance, as individuals continuously attempt to detect possible indicators of illness. In older adults, this relationship may be particularly pronounced. Aging is associated with numerous physiological changes and reduced immune functioning, which increase the frequency and salience of bodily sensations (8). These changes can intensify health-related concerns and provide a constant source of bodily cues that attract attention. As a result, individuals with higher levels of health anxiety may be more likely to interpret these normal age-related sensations as signs of serious illness, thereby reinforcing continuous monitoring of the body. From a cognitive perspective, health anxiety is also associated with dysfunctional health-related beliefs, including overestimation of the likelihood of illness, fear of illness, perceived inability to cope with disease, and doubts about the effectiveness of medical care (27). These maladaptive beliefs contribute to increased vigilance toward bodily sensations, as individuals attempt to achieve certainty about their health status. However, this heightened focus on the body does not reduce anxiety; rather, it maintains and intensifies it by increasing awareness of bodily sensations that may otherwise be ignored.
The fourth hypothesis proposed that bodily vigilance mediates the relationship between health anxiety and illness perception in older adults. The findings of the present study confirmed this hypothesis, indicating that bodily vigilance plays a significant mediating role in this relationship. In other words, health anxiety not only exerts a direct effect on illness perception, but also influences illness perception indirectly through increased attentional focus on bodily sensations. This suggests that older adults with higher levels of health anxiety are more likely to engage in excessive monitoring of their bodily states, which in turn contributes to more negative and intensified perceptions of illness. This finding can be understood within the conceptualization of health anxiety as a condition characterized by the misinterpretation of bodily sensations or physical changes as signs of serious illness (24). Individuals with health anxiety are preoccupied with the belief that they are suffering from a physical disease, which increases their attention to internal bodily cues. This heightened attentional focus constitutes bodily vigilance, which serves as a cognitive mechanism through which health anxiety is translated into illness perception. In line with Leventhal’s self-regulation model, illness perception is shaped by individuals’ cognitive representations of symptoms, perceived consequences, and controllability of illness (13). Accordingly, when bodily sensations are continuously monitored and selectively attended to, they are more likely to be incorporated into these cognitive representations. In older adults, this process may be particularly pronounced due to age-related physiological changes, increased frequency of somatic experiences, and reduced physical resilience (8). These conditions make bodily sensations more salient and more likely to be interpreted as indicators of illness.
Furthermore, health anxiety involves dysfunctional beliefs about the likelihood of illness, fear of disease, perceived inability to cope with illness, and doubts regarding medical reassurance (27). These maladaptive beliefs intensify attention toward bodily sensations and increase the tendency to interpret ambiguous physical cues as threatening. As a result, bodily vigilance becomes a central pathway through which cognitive and emotional concerns about health are transformed into illness-related interpretations. Within this framework, bodily vigilance acts as a mediating cognitive process that links emotional vulnerability (health anxiety) to cognitive outcomes (illness perception). As individuals increasingly monitor their internal bodily states, they become more likely to detect normal physiological sensations, which are then interpreted through the lens of health-related fears.
Conclusion
The findings indicated that health anxiety had a significant positive effect on both bodily vigilance and illness perception, and bodily vigilance also significantly predicted illness perception. In addition, bodily vigilance was confirmed as a significant mediator in the relationship between health anxiety and illness perception. These results suggest that illness perception in older adults is shaped through both direct emotional-cognitive processes and indirect attentional mechanisms. From a theoretical perspective, the findings support cognitive-behavioral models of health anxiety, emphasizing the role of maladaptive beliefs and attentional bias toward bodily sensations. Practically, the results highlight the importance of targeting both health anxiety and excessive body monitoring in psychological interventions for older adults.
Study limitations
This study had some limitations. The cross-sectional design limits causal interpretations, and the use of convenience sampling restricts generalizability. In addition, reliance on self-report measures may have introduced bias, and medical variables such as comorbidities were not controlled. In terms of practical implications, it is recommended that health professionals screen for health anxiety in the elderly populations and use interventions such as cognitive-behavioral therapy to reduce maladaptive health beliefs and bodily hypervigilance. Future research should employ longitudinal designs and broader samples to better clarify causal relationships among these variables. In addition, participants were recruited from clinical settings without formal diagnostic screening for health anxiety. Therefore, the sample may include individuals with varying levels of health anxiety rather than clinically diagnosed cases, which should be considered when interpreting the findings. Furthermore, due to the use of interviewer-administered questionnaires for some participants, the possibility of interviewer bias and social desirability bias cannot be completely ruled out. Although standardized administration procedures were applied to minimize these effects, future studies are recommended to use multiple trained interviewers and to assess inter-rater reliability. Another limitation of the present study is the absence of inter-rater reliability assessment, as data coding and analysis were conducted by a single researcher.
Conflict of interests
The authors declare no conflict if interests.
Acknowledgments
The authors sincerely appreciate the participation of all elderly individuals in this study.
Funding
None
Authors' contributions
S.M. Conceptualization, Data Curation, Formal Analysis, Investigation, Writing – Original Draft. E.G. Methodology, Validation, Writing – Review & Editing. K.B. Investigation, Resources, Literature Review, Writing – Review & Editing. M.G. Conceptualization, Supervision, Project Administration, Validation, Writing – Review & Editing. All authors read and approved the final manuscript and agreed to be accountable for all aspects of the work.
References
- Dharmarajan T. Physiology of aging. In: Pitchumoni CS, Dharmarajan T, editors. Geriatric gastroenterology. Springer: 2021; P. 101-53.
- Shakkarpude J, Jesse AD, Kumar P, Kumar R. Physiology of Aging. In: Principles of Veterinary Animal Physiology. CRC Press; 2025. p. 242-52.
- Guo J, Huang X, Dou L, Yan M, Shen T, Tang W, et al. Aging and aging-related diseases: from molecular mechanisms to interventions and treatments. Signal Transduction and Targeted Therapy. 2022; 7(1): 1-40.
- Bhandari P, Paswan B. Lifestyle behaviours and mental health outcomes of elderly: Modification of socio-economic and physical health effects. Ageing International. 2021; 46(1): 35-69.
- Xu X, Zhang L. How does childhood socio-economic environment affect the health of middle-aged and elderly people in China? A new perspective with four dimensions of health. Journal of Public Health. 2023; 31(8): 1249-58.
- McKenna-Plumley PE, Turner RN, Yang K, Groarke JM. “It’sa feeling of complete disconnection”: experiences of existential loneliness from youth to older adulthood. BMC Psychology. 2023; 11(1): 1-14.
- Alsenany SA. Psychological predictors of gerascophobia among middle-aged and older adults: the role of health anxiety and body image satisfaction. GeroScience. 2026; 48(2): 2681-93.
- Howell C, Segal DL, Segal S. Diagnosis and assessment of somatic symptom and related disorders among older adults: Issues and strategies. Journal of Clinical and Basic Psychosomatics. 2025; 3(4): 21-9.
- Xiong C, Jiang C, Zhang H, Chen J, Zhao M, Xiong C, Luo X, et al. Self‐management and illness perception among cervical cancer patients: A cross‐sectional study. International Journal of Nursing Practice. 2023; 29(3): 13134.
- Singh A, Rejeb A. Illness perception: a bibliometric study. Heliyon. 2024; 10(11(: 1-26.
- Scollan-Koliopoulos M. Lifestyle r-educing program: risk–education in groups with depression to prevent diabetes. Regis College; 2022.
- Bilondi SS, Noghabi AD, Aalami H. The relationship between illness perception and medication adherence in patients with diabetes mellitus type II: illness perception and medication adherence. Journal of Preventive Medicine and Hygiene. 2022; 62(4): 966-71.
- Leventhal H, Halm E, Horowitz C, Leventhal EA, Ozakinci G. Living with chronic illness: A contextualized, self-regulation approach. The Sage Handbook of Health Psychology. 2004: 197-240.
- Ma H, Hu K, Wu W, Wu Q, Ye Q, Jiang X, et al. Illness perception profile among cancer patients and its influencing factors: A cross-sectional study. European Journal of Oncology Nursing. 2024; 69: 102526.
- Fournier H, Calcagni N, Morice-Picard F, Quintard B. Psychosocial implications of rare genetic skin diseases affecting appearance on daily life experiences, emotional state, self-perception and quality of life in adults: a systematic review. Orphanet Journal of Rare Diseases. 2023; 18(1): 1-49.
- Nie R, Han Y, Xu J, Huang Q, Mao J. Illness perception, risk perception and health promotion self-care behaviors among Chinese patient with type 2 diabetes: A cross-sectional survey. Applied Nursing Research. 2018; 39: 89-96.
- de Santana Silva JP, Cruz HRA, Silva GAG, Gualdi LP, Lima ÍNDF. Illness perception and self-care in hypertension treatment: a scoping review of current literature. BMC Health Services Research. 2024; 24(1): 1-14.
- Zhu Y, Cai N, Wang Z, Li J, Guo T, He J, et al. Perceived social support and psychosocial adaptation in patients with chronic skin diseases: the mediating role of self-disclosure. Frontiers in Psychiatry. 2025; 16: 1-16.
- Bassi M, Falautano M, Cilia S, Goretti B, Grobberio M, Pattini M, et al. Illness perception and well-being among persons with multiple sclerosis and their caregivers. Journal of Clinical Psychology in Medical Settings. 2016; 23(1): 33-52.
- Ośmiałowska E, Staś J, Chabowski M, Jankowska-Polańska B. Illness perception and quality of life in patients with breast cancer. Cancers. 2022; 14(5): 1-22.
- Lebel S, Mutsaers B, Tomei C, Leclair CS, Jones G, Petricone-Westwood D, et al. Health anxiety and illness-related fears across diverse chronic illnesses: A systematic review on conceptualization, measurement, prevalence, course, and correlates. Plos One. 2020; 15(7): 1.-48
- Bulut BP, Bozo Ö. A helix of anxiety: a qualitative analysis of the personal experiences of individuals with health anxiety. Studies in Psychology. 2022; 42(1): 165-98.
- Axelsson E, Hedman-Lagerlöf E. Validity and clinical utility of distinguishing between DSM-5 somatic symptom disorder and illness anxiety disorder in pathological health anxiety: Should we close the chapter? Journal of Psychosomatic Research. 2023; 165: 111133.
- Ferguson E. A taxometric analysis of health anxiety. Psychological Medicine. 2009; 39(2): 277-85.
- Salkovskis PM, Rimes KA, Warwick HM, Clark D. The health anxiety inventory: development and validation of scales for the measurement of health anxiety and hypochondriasis. Psychological Medicine. 2002; 32(5): 843-53.
- Weck F, Richtberg S, MB Neng J. Epidemiology of hypochondriasis and health anxiety: comparison of different diagnostic criteria. Current Psychiatry Reviews. 2014; 10(1): 14-23.
- Salkovskis PM, Warwick HM. Morbid preoccupations, health anxiety and reassurance: a cognitive-behavioural approach to hypochondriasis. Behaviour Research and Therapy. 1986; 24(5): 597-602.
- Hannah K, Marie K, Olaf H, Stephan B, Andreas D, Wilson Michael L, et al. The global economic burden of health anxiety/hypochondriasis-a systematic review. BMC Public Health. 2023; 23(1): 1-11.
- Rachman S. Health anxiety disorders: A cognitive construal. Behaviour Research and Therapy. 2012; 50(7-8): 502-12.
- Bailer J, Kerstner T, Witthöft M, Diener C, Mier D, Rist F. Health anxiety and hypochondriasis in the light of DSM-5. Anxiety, Stress, & Coping. 2016; 29(2): 219-39.
- Sauer KS, Witthöft M, Rief W. Somatic symptom disorder and health anxiety: assessment and management. Neurologic Clinics. 2023; 41(4): 745-58.
- Tyrer P. Recent advances in the understanding and treatment of health anxiety. Current Psychiatry Reports. 2018; 20(7): 49.
- Wheaton MG, Berman NC, Abramowitz JS. The contribution of experiential avoidance and anxiety sensitivity in the prediction of health anxiety. Journal of Cognitive Psychotherapy. 2010; 24(3): 229.
- Schmidt NB, Lerew DR, Trakowski JH. Body vigilance in panic disorder: evaluating attention to bodily perturbations. Journal of Consulting and Clinical Psychology. 1997; 65(2): 214.
- McLaughlin LE, McLeish AC, O'Bryan EM. The role of body vigilance in depression symptomatology. International Journal of Cognitive Therapy. 2016; 9(3): 217-28.
- Zvolensky MJ, Kauffman BY, Shepherd JM, Viana AG, Bogiaizian D, Rogers AH, et al. Pain-related anxiety among Latinx college students: relations to body vigilance, worry, anxious arousal, and general depression. Journal of Racial and Ethnic Health Disparities. 2020; 7(3): 498-507.
- Ginzburg K, Tsur N, Barak-Nahum A, Defrin R. Body awareness: differentiating between sensitivity to and monitoring of bodily signals. Journal of Behavioral Medicine. 2014; 37(3): 564-75.
- Wright EC, Hostinar CE, Trainor BC. Anxious to see you: Neuroendocrine mechanisms of social vigilance and anxiety during adolescence. The European Journal of Neuroscience. 2020; 52(1): 2516-29.
- Sutton R, de Jong JS, Stewart JM, Fedorowski A, de Lange FJ. Pacing in vasovagal syncope: physiology, pacemaker sensors, and recent clinical trials—precise patient selection and measurable benefit. Heart Rhythm. 2020; 17(5): 821-8.
- Hedman E, Lekander M, Karshikoff B, Ljótsson B, Axelsson E, Axelsson J. Health anxiety in a disease-avoidance framework: Investigation of anxiety, disgust and disease perception in response to sickness cues. Journal of Abnormal Psychology. 2016; 125(7): 868-78.
- Hayter AL, Salkovskis PM, Silber E, Morris RG. The impact of health anxiety in patients with relapsing remitting multiple sclerosis: Misperception, misattribution and quality of life. The British Journal of Clinical Psychology. 2016; 55(4): 371-86.
- Kline RB. Principles and practice of structural equation modeling. New York: London: Guilford publications; 2023.
- Abramowitz JS, Olatunji BO, Deacon BJ. Health anxiety, hypochondriasis, and the anxiety disorders. Behavior Therapy. 2007; 38(1): 86-94.
- Nargesi F, Izadi F, Kariminejad K, Rezaii Sharif A. The investigation of the reliability and validity of Persian version of Health anxiety questionnaire in students of Lorestan University of Medical Sciences. Quarterly of Educational Measurement. 2017; 8(27): 147-160. [Persian]
- Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. Journal of Psychosomatic Research. 2006; 60(6): 631-7.
- Karimian Z, Haghayegh SA, Emami Najafi Dehkordi S MH, Raisi M. The Comparison of the effectiveness of trans-diagnostic treatment and the acceptance and commitment therapy (ACT) on Emotion regulation and illness perception in patients with irritable bowel syndrome (IBS). Journal of Research in Behavioural Sciences. 2021; 19(3): 477-88. [Persian]
- Hair JF, Risher JJ, Sarstedt M, Ringle CM. When to use and how to report the results of PLS-SEM. European Business Review. 2019; 31(1): 2-4.
- Myers JL, Well AD, Lorch Jr, Robert F. Research design and statistical analysis. Routledge; 2013.
- Lomax RG. A beginner's guide to structural equation modeling. psychology press; 2004.
Type of Study: Research |
Subject:
Special
Received: 2026/04/21 | Accepted: 2026/06/8 | Published: 2026/06/20
Received: 2026/04/21 | Accepted: 2026/06/8 | Published: 2026/06/20
References
1. Dharmarajan T. Physiology of aging. In: Pitchumoni CS, Dharmarajan T, editors. Geriatric gastroenterology. Springer: 2021; P. 101-53.
2. Shakkarpude J, Jesse AD, Kumar P, Kumar R. Physiology of Aging. In: Principles of Veterinary Animal Physiology. CRC Press; 2025. p. 242-52.
3. Guo J, Huang X, Dou L, Yan M, Shen T, Tang W, et al. Aging and aging-related diseases: from molecular mechanisms to interventions and treatments. Signal Transduction and Targeted Therapy. 2022; 7(1): 1-40.
4. Bhandari P, Paswan B. Lifestyle behaviours and mental health outcomes of elderly: Modification of socio-economic and physical health effects. Ageing International. 2021; 46(1): 35-69.
5. Xu X, Zhang L. How does childhood socio-economic environment affect the health of middle-aged and elderly people in China? A new perspective with four dimensions of health. Journal of Public Health. 2023; 31(8): 1249-58.
6. McKenna-Plumley PE, Turner RN, Yang K, Groarke JM. “It’sa feeling of complete disconnection”: experiences of existential loneliness from youth to older adulthood. BMC Psychology. 2023; 11(1): 1-14.
7. Alsenany SA. Psychological predictors of gerascophobia among middle-aged and older adults: the role of health anxiety and body image satisfaction. GeroScience. 2026; 48(2): 2681-93.
8. Howell C, Segal DL, Segal S. Diagnosis and assessment of somatic symptom and related disorders among older adults: Issues and strategies. Journal of Clinical and Basic Psychosomatics. 2025; 3(4): 21-9.
9. Xiong C, Jiang C, Zhang H, Chen J, Zhao M, Xiong C, Luo X, et al. Self‐management and illness perception among cervical cancer patients: A cross‐sectional study. International Journal of Nursing Practice. 2023; 29(3): 13134.
10. Singh A, Rejeb A. Illness perception: a bibliometric study. Heliyon. 2024; 10(11(: 1-26.
11. Scollan-Koliopoulos M. Lifestyle r-educing program: risk–education in groups with depression to prevent diabetes. Regis College; 2022.
12. Bilondi SS, Noghabi AD, Aalami H. The relationship between illness perception and medication adherence in patients with diabetes mellitus type II: illness perception and medication adherence. Journal of Preventive Medicine and Hygiene. 2022; 62(4): 966-71.
13. Leventhal H, Halm E, Horowitz C, Leventhal EA, Ozakinci G. Living with chronic illness: A contextualized, self-regulation approach. The Sage Handbook of Health Psychology. 2004: 197-240.
14. Ma H, Hu K, Wu W, Wu Q, Ye Q, Jiang X, et al. Illness perception profile among cancer patients and its influencing factors: A cross-sectional study. European Journal of Oncology Nursing. 2024; 69: 102526.
15. Fournier H, Calcagni N, Morice-Picard F, Quintard B. Psychosocial implications of rare genetic skin diseases affecting appearance on daily life experiences, emotional state, self-perception and quality of life in adults: a systematic review. Orphanet Journal of Rare Diseases. 2023; 18(1): 1-49.
16. Nie R, Han Y, Xu J, Huang Q, Mao J. Illness perception, risk perception and health promotion self-care behaviors among Chinese patient with type 2 diabetes: A cross-sectional survey. Applied Nursing Research. 2018; 39: 89-96.
17. de Santana Silva JP, Cruz HRA, Silva GAG, Gualdi LP, Lima ÍNDF. Illness perception and self-care in hypertension treatment: a scoping review of current literature. BMC Health Services Research. 2024; 24(1): 1-14.
18. Zhu Y, Cai N, Wang Z, Li J, Guo T, He J, et al. Perceived social support and psychosocial adaptation in patients with chronic skin diseases: the mediating role of self-disclosure. Frontiers in Psychiatry. 2025; 16: 1-16.
19. Bassi M, Falautano M, Cilia S, Goretti B, Grobberio M, Pattini M, et al. Illness perception and well-being among persons with multiple sclerosis and their caregivers. Journal of Clinical Psychology in Medical Settings. 2016; 23(1): 33-52.
20. Ośmiałowska E, Staś J, Chabowski M, Jankowska-Polańska B. Illness perception and quality of life in patients with breast cancer. Cancers. 2022; 14(5): 1-22.
21. Lebel S, Mutsaers B, Tomei C, Leclair CS, Jones G, Petricone-Westwood D, et al. Health anxiety and illness-related fears across diverse chronic illnesses: A systematic review on conceptualization, measurement, prevalence, course, and correlates. Plos One. 2020; 15(7): 1.-48
22. Bulut BP, Bozo Ö. A helix of anxiety: a qualitative analysis of the personal experiences of individuals with health anxiety. Studies in Psychology. 2022; 42(1): 165-98.
23. Axelsson E, Hedman-Lagerlöf E. Validity and clinical utility of distinguishing between DSM-5 somatic symptom disorder and illness anxiety disorder in pathological health anxiety: Should we close the chapter? Journal of Psychosomatic Research. 2023; 165: 111133.
24. Ferguson E. A taxometric analysis of health anxiety. Psychological Medicine. 2009; 39(2): 277-85.
25. Salkovskis PM, Rimes KA, Warwick HM, Clark D. The health anxiety inventory: development and validation of scales for the measurement of health anxiety and hypochondriasis. Psychological Medicine. 2002; 32(5): 843-53.
26. Weck F, Richtberg S, MB Neng J. Epidemiology of hypochondriasis and health anxiety: comparison of different diagnostic criteria. Current Psychiatry Reviews. 2014; 10(1): 14-23.
27. Salkovskis PM, Warwick HM. Morbid preoccupations, health anxiety and reassurance: a cognitive-behavioural approach to hypochondriasis. Behaviour Research and Therapy. 1986; 24(5): 597-602.
28. Hannah K, Marie K, Olaf H, Stephan B, Andreas D, Wilson Michael L, et al. The global economic burden of health anxiety/hypochondriasis-a systematic review. BMC Public Health. 2023; 23(1): 1-11.
29. Rachman S. Health anxiety disorders: A cognitive construal. Behaviour Research and Therapy. 2012; 50(7-8): 502-12.
30. Bailer J, Kerstner T, Witthöft M, Diener C, Mier D, Rist F. Health anxiety and hypochondriasis in the light of DSM-5. Anxiety, Stress, & Coping. 2016; 29(2): 219-39.
31. Sauer KS, Witthöft M, Rief W. Somatic symptom disorder and health anxiety: assessment and management. Neurologic Clinics. 2023; 41(4): 745-58.
32. Tyrer P. Recent advances in the understanding and treatment of health anxiety. Current Psychiatry Reports. 2018; 20(7): 49.
33. Wheaton MG, Berman NC, Abramowitz JS. The contribution of experiential avoidance and anxiety sensitivity in the prediction of health anxiety. Journal of Cognitive Psychotherapy. 2010; 24(3): 229.
34. Schmidt NB, Lerew DR, Trakowski JH. Body vigilance in panic disorder: evaluating attention to bodily perturbations. Journal of Consulting and Clinical Psychology. 1997; 65(2): 214.
35. McLaughlin LE, McLeish AC, O'Bryan EM. The role of body vigilance in depression symptomatology. International Journal of Cognitive Therapy. 2016; 9(3): 217-28.
36. Zvolensky MJ, Kauffman BY, Shepherd JM, Viana AG, Bogiaizian D, Rogers AH, et al. Pain-related anxiety among Latinx college students: relations to body vigilance, worry, anxious arousal, and general depression. Journal of Racial and Ethnic Health Disparities. 2020; 7(3): 498-507.
37. Ginzburg K, Tsur N, Barak-Nahum A, Defrin R. Body awareness: differentiating between sensitivity to and monitoring of bodily signals. Journal of Behavioral Medicine. 2014; 37(3): 564-75.
38. Wright EC, Hostinar CE, Trainor BC. Anxious to see you: Neuroendocrine mechanisms of social vigilance and anxiety during adolescence. The European Journal of Neuroscience. 2020; 52(1): 2516-29.
39. Sutton R, de Jong JS, Stewart JM, Fedorowski A, de Lange FJ. Pacing in vasovagal syncope: physiology, pacemaker sensors, and recent clinical trials—precise patient selection and measurable benefit. Heart Rhythm. 2020; 17(5): 821-8.
40. Hedman E, Lekander M, Karshikoff B, Ljótsson B, Axelsson E, Axelsson J. Health anxiety in a disease-avoidance framework: Investigation of anxiety, disgust and disease perception in response to sickness cues. Journal of Abnormal Psychology. 2016; 125(7): 868-78.
41. Hayter AL, Salkovskis PM, Silber E, Morris RG. The impact of health anxiety in patients with relapsing remitting multiple sclerosis: Misperception, misattribution and quality of life. The British Journal of Clinical Psychology. 2016; 55(4): 371-86.
42. Kline RB. Principles and practice of structural equation modeling. New York: London: Guilford publications; 2023.
43. Abramowitz JS, Olatunji BO, Deacon BJ. Health anxiety, hypochondriasis, and the anxiety disorders. Behavior Therapy. 2007; 38(1): 86-94.
44. Nargesi F, Izadi F, Kariminejad K, Rezaii Sharif A. The investigation of the reliability and validity of Persian version of Health anxiety questionnaire in students of Lorestan University of Medical Sciences. Quarterly of Educational Measurement. 2017; 8(27): 147-160. [Persian]
45. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. Journal of Psychosomatic Research. 2006; 60(6): 631-7.
46. Karimian Z, Haghayegh SA, Emami Najafi Dehkordi S MH, Raisi M. The Comparison of the effectiveness of trans-diagnostic treatment and the acceptance and commitment therapy (ACT) on Emotion regulation and illness perception in patients with irritable bowel syndrome (IBS). Journal of Research in Behavioural Sciences. 2021; 19(3): 477-88. [Persian]
47. Hair JF, Risher JJ, Sarstedt M, Ringle CM. When to use and how to report the results of PLS-SEM. European Business Review. 2019; 31(1): 2-4.
48. Myers JL, Well AD, Lorch Jr, Robert F. Research design and statistical analysis. Routledge; 2013.
49. Lomax RG. A beginner's guide to structural equation modeling. psychology press; 2004.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
