

Volume 12, Issue 1 (June 2026)
Elderly Health Journal 2026, 12(1): 80-93 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sharma D. Yogic Dietary Interventions for Nutritional Health and Well-Being in Older Adults: A Systematic Review and Conceptual Framework. Elderly Health Journal 2026; 12 (1) :80-93
URL: http://ehj.ssu.ac.ir/article-1-381-en.html
URL: http://ehj.ssu.ac.ir/article-1-381-en.html



School of Buddhist Studies, Philosophy & Comparative Religions / School of Languages and Literature/Humanities, Nalanda University, Rajgir, Bihar, India , mdivyarkl@gmail.com
Full-Text [PDF 647 kb]
(33 Downloads)
| Abstract (HTML) (338 Views)
Table 1. Methodological quality assessment summary
Table 2. Adherence reporting across included studies
N/A = not applicable (cross-sectional observational studies). Adherence rates extracted from study reports; adequate adherence defined as ≥80% completion of prescribed sessions or meal protocols where reported.
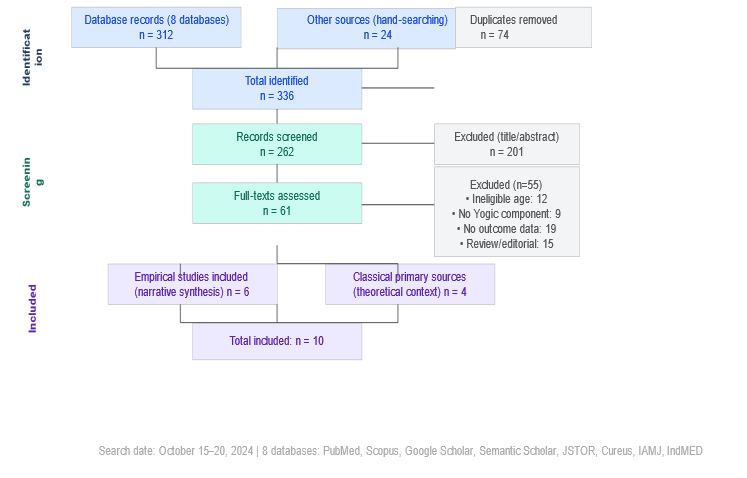
Figure 1. PRISMA 2020 flow diagram for systematic search and study selection, illustrating the number of records identified, screened, assessed for eligibility, and included at each stage of the review process.
Table 3. Characteristics of included empirical studies
Table 4. MNA/MNA-SF outcome data across interventional studies reporting nutritional status measurements
*95% CI calculated using normal approximation: SE = SD/√n, with n = 30.
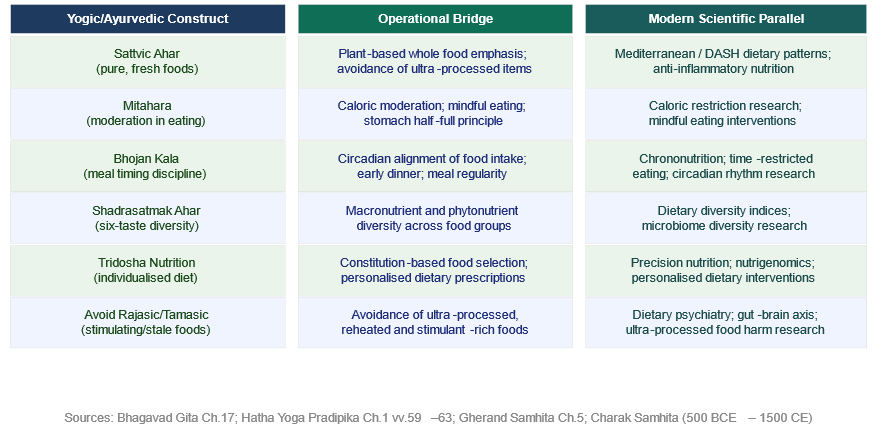
Figure 2. Conceptual Alignment Between Yogic Dietary Philosophy and Contemporary Evidence-Based Nutritional Science. This framework illustrates substantive congruence between classical Yogic dietary constructs (developed approximately 500 BCE to 1500 CE) and modern nutritional science paradigms, supporting the translational validity of Yogic dietary interventions in geriatric care.
Table 5. The Panchakosha-Nutritional Integration Model: Mapping Classical Yogic Constructs onto Modern Nutritional Science Domains
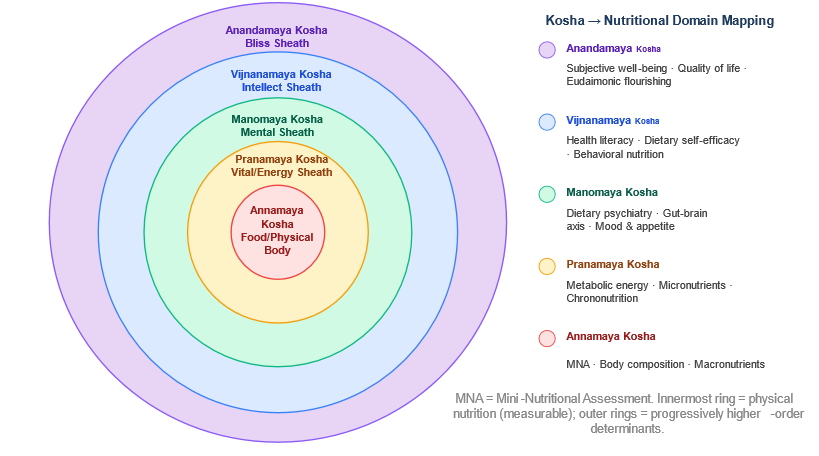
Figure 3. The Panchakosha-Nutritional Integration Model. Concentric circles representing the five Koshas (sheaths) of the Yogic framework, from innermost (Annamaya Kosha: physical nutrition) to outermost (Anandamaya Kosha: bliss/well-being), each mapped to its corresponding modern nutritional science domain. The model provides a theoretical basis for holistic, multi-dimensional nutritional assessment in older adults.
Full-Text: (22 Views)
Yogic Dietary Interventions for Nutritional Health and Well-Being in Older Adults: A Systematic Review and Conceptual Framework
Divya Sharma 1*
Article history
Received 3 May 2026
Accepted 14 June 2026
A B S T R A C T
Introduction: Geriatric malnutrition is a pervasive clinical and public health challenge linked to functional decline, increased hospitalization rates, and diminished quality of life. Traditional Indian dietary systems, rooted in the classical frameworks of Yoga and Ayurveda, offer structured, culturally embedded philosophical approaches to nutritional management in older adults. Despite growing scholarly and clinical interest, the evidence base for Yogic dietary interventions in geriatric populations has not yet been formally synthesized.
Methods: A systematic literature search was conducted across PubMed/MEDLINE, ScienceDirect, Google Scholar, Semantic Scholar, JSTOR, and Indian databases (IAMJ, IndMED, Cureus), supplemented by hand-searching classical primary sources. Studies enrolling community-dwelling older adults who received Yogic or Ayurvedic dietary interventions and reported validated nutritional outcomes were eligible. Two reviewers independently screened records, extracted data, and assessed methodological quality.
Results: Six empirical studies and four classical textual sources were included. Yogic dietary interventions consistently improved Mini-Nutritional Assessment (MNA) scores across studies. Two RCTs and two pre-post interventional studies demonstrated consistent improvements in MNA scores and malnutrition risk reduction following dietary and nutrition education interventions. The methodologically strongest available Indian evidence demonstrated a rise in mean MNA from 21.4 ± 1.12 to 23.15 ± 1.71 (p < 0.001), substantially improving mean MNA scores from the at-risk range (21.4) to near the normal threshold (23.15). A community-based interventional study (n = 205) confirmed a significant reduction in malnutrition prevalence from 40.5% to 30.7% (p < 0.05). A novel Panchakosha-Nutritional Integration Model is proposed, mapping classical Yogic constructs onto five modern nutritional and well-being domains.
Conclusion: Yogic dietary interventions appear to be associated with improved nutritional well-being in older adults, though causal inference is limited by the observational nature of most included studies. The proposed Panchakosha model offers a translational framework for integrating these ancient principles into geriatric nutrition research and practice. Larger, multi-centre trials incorporating biochemical markers and extended follow-up are recommended.
Keywords: Yogic Diet, Malnutrition, Circadian Nutrition, Systematic Review, Ayurveda
Introduction
Divya Sharma 1*
- School of Buddhist Studies, Philosophy & Comparative Religions / School of Languages and Literature/Humanities, Nalanda University, Rajgir, Bihar, India
Article history
Received 3 May 2026
Accepted 14 June 2026
A B S T R A C T
Introduction: Geriatric malnutrition is a pervasive clinical and public health challenge linked to functional decline, increased hospitalization rates, and diminished quality of life. Traditional Indian dietary systems, rooted in the classical frameworks of Yoga and Ayurveda, offer structured, culturally embedded philosophical approaches to nutritional management in older adults. Despite growing scholarly and clinical interest, the evidence base for Yogic dietary interventions in geriatric populations has not yet been formally synthesized.
Methods: A systematic literature search was conducted across PubMed/MEDLINE, ScienceDirect, Google Scholar, Semantic Scholar, JSTOR, and Indian databases (IAMJ, IndMED, Cureus), supplemented by hand-searching classical primary sources. Studies enrolling community-dwelling older adults who received Yogic or Ayurvedic dietary interventions and reported validated nutritional outcomes were eligible. Two reviewers independently screened records, extracted data, and assessed methodological quality.
Results: Six empirical studies and four classical textual sources were included. Yogic dietary interventions consistently improved Mini-Nutritional Assessment (MNA) scores across studies. Two RCTs and two pre-post interventional studies demonstrated consistent improvements in MNA scores and malnutrition risk reduction following dietary and nutrition education interventions. The methodologically strongest available Indian evidence demonstrated a rise in mean MNA from 21.4 ± 1.12 to 23.15 ± 1.71 (p < 0.001), substantially improving mean MNA scores from the at-risk range (21.4) to near the normal threshold (23.15). A community-based interventional study (n = 205) confirmed a significant reduction in malnutrition prevalence from 40.5% to 30.7% (p < 0.05). A novel Panchakosha-Nutritional Integration Model is proposed, mapping classical Yogic constructs onto five modern nutritional and well-being domains.
Conclusion: Yogic dietary interventions appear to be associated with improved nutritional well-being in older adults, though causal inference is limited by the observational nature of most included studies. The proposed Panchakosha model offers a translational framework for integrating these ancient principles into geriatric nutrition research and practice. Larger, multi-centre trials incorporating biochemical markers and extended follow-up are recommended.
Keywords: Yogic Diet, Malnutrition, Circadian Nutrition, Systematic Review, Ayurveda
Copyright © 2026 The Author(s). This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/) which permits copy and redistribute the material just in noncommercial usages, provided the original work is properly cite.
Introduction
The global population aged 60 years and above is projected to exceed 2.1 billion by 2050, representing one of the most consequential demographic transitions in recorded history (1). Embedded within this transition is an escalating burden of geriatric malnutrition, a condition characterized primarily by insufficient intake of energy, protein, and micronutrients relative to physiological requirements, leading to measurable deterioration in body composition and functional capacity (2, 3). Malnutrition affects between 15% and 60% of community-dwelling older adults depending on the setting and assessment methodology employed, and constitutes a major independent predictor of frailty, falls, cognitive decline, increased hospitalization, and premature mortality (4-6).
Diet remains one of the most powerful and modifiable determinants of health across the life course, and its clinical significance intensifies with advancing age (7). Age-related physiological changes (reduced appetite, dental deterioration, altered gastrointestinal motility, diminished taste sensitivity, and impaired nutrient absorption) interact dynamically with psychosocial adversities such as social isolation, depression, bereavement, and economic constraint to erode dietary adequacy in older populations (8, 9). Emerging evidence in psychiatric nutrition and nutritional neuroscience further suggests that dietary quality exerts bidirectional influence on mental health outcomes, including the risk of late-life depression, anxiety, and dementia, conditions that themselves contribute to nutritional vulnerability in a vicious cycle (10-12).
Against this backdrop, the traditional dietary systems of India offer a body of knowledge that is both ancient in provenance and strikingly contemporary in its implications. Yoga and Ayurveda, the principal classical Indian life sciences, articulate comprehensive frameworks for dietary management that address not merely the biochemical composition of food, but also its preparation, timing, quantity, sensory qualities, and psycho-spiritual context of consumption (13-15). The Yogic dietary philosophy centers on three foundational constructs: Sattvic Ahar (pure, fresh, plant-predominant foods that promote clarity and vitality), Mitahara (the disciplined practice of eating in moderation, consuming meals until the stomach is approximately half full), and Bhojan Kala (the prescription of specific meal timings aligned with circadian biological rhythms) (16, 17). The Ayurvedic extension of this framework introduces concepts of Shadrasatmak Ahar (dietary diversity encompassing all six tastes), Ahar Matra (appropriate food quantity calibrated to digestive capacity), and tridoshic balance (individualized dietary prescription according to constitutional type) (18).
Remarkably, each of these ancient constructs finds meaningful parallel in contemporary nutritional science: Sattvic Ahar overlaps substantially with the Mediterranean and Dietary Approaches to Stop Hypertension (DASH) dietary patterns; Mitahara resonates with the principles of caloric restriction and mindful eating; Bhojan Kala anticipates the emerging discipline of chrononutrition; Shadrasatmak Ahar aligns with dietary diversity indices associated with microbiome health; and tridoshic nutrition foreshadows the precision nutrition paradigm (19, 20). These convergences are not coincidental; they represent the independent distillation of empirical dietary wisdom accumulated over several millennia of systematic human observation.
Despite a substantial volume of literature on geriatric malnutrition and the clinical benefits of structured dietary interventions, no systematic review has yet synthesized the available evidence on Yogic dietary frameworks specifically applied to older adult populations. This represents a significant gap in the scientific literature, particularly given the scale of the aging population in South and Southeast Asia, where Yogic and Ayurvedic traditions retain deep cultural salience and practical accessibility. This review aims to address that gap directly.
In addition to synthesizing the empirical evidence, this review offers a novel theoretical contribution: the Panchakosha-Nutritional Integration Model, which maps the five classical Yogic sheaths of existence (Koshas) onto corresponding domains of modern nutritional science, providing a conceptual framework for the systematic study and clinical application of Yogic dietary interventions across the full spectrum of geriatric health and well-being.
This systematic review had two primary objectives: (i) to identify, appraise, and synthesize empirical evidence on the effects of Yogic dietary interventions on nutritional status and related well-being outcomes in adults aged 60 years and above; and (ii) to propose and elaborate a novel conceptual framework, the Panchakosha-Nutritional Integration Model, that bridges classical Yogic epistemology with contemporary nutritional science to guide future research and clinical practice.
Methods
Review design, registration, and PRISMA reporting
This systematic review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The review protocol was retrospectively registered on the Open Science Framework (OSF) following completion of data extraction. (Registration: https://osf.io/r42h5/overview?view_only=8aa7c085416e4e4f92265c33656ad90c).
While prospective PROSPERO registration was not completed prior to data extraction, which is a recognized limitation, the OSF registration provides a time-stamped protocol record. The absence of prospective registration is reported transparently in accordance with PRISMA 2020 guidance and is addressed in the limitations section of the Discussion.
Search strategy
A comprehensive, systematic electronic literature search was conducted across eight databases: PubMed/MEDLINE, ScienceDirect, Google Scholar, Semantic Scholar, JSTOR, Cureus, the International Ayurvedic Medical Journal (IAMJ), and IndMED (the Indian medical database). The search was performed between October 15 and 20, 2024, with no lower date restriction applied. One included study (Meena et al., 2025) was identified through a hand search of the Cureus database, where it appeared as an online-first publication ahead of formal print assignment; accordingly, it is cited using its 2025 final publication year.. Search terms were constructed using Boolean operators across three concept domains: (“Yogic diet” OR “Sattvic diet” OR “Mitahara” OR “Ayurvedic diet” OR “traditional Indian diet” OR “Sattvic Ahar” OR “Bhojan Kala”) AND (“elderly” OR “older adults” OR “geriatric” OR “aged” OR “aging” OR “senior”) AND (“nutrition” OR “nutritional status” OR “malnutrition” OR “dietary intervention” OR “well-being” OR “appetite” OR “sleep” OR “bowel function”). The complete PubMed search string is provided as Supplementary Material (Appendix S1). Example PubMed string: ("Yogic diet"[tiab] OR "Sattvic diet"[tiab] OR "Mitahara"[tiab] OR "Ayurvedic diet"[tiab]) AND ("elderly"[tiab] OR "older adults"[tiab] OR "geriatric"[tiab] OR "aged"[MeSH]) AND ("nutrition"[tiab] OR "nutritional status"[tiab] OR "malnutrition"[tiab] OR "dietary intervention"[tiab]). JSTOR was included specifically to facilitate identification of classical primary textual sources not indexed in clinical databases. Grey literature sources (ProQuest Dissertations, conference proceedings) were not systematically searched; this is acknowledged as a limitation, as relevant unpublished studies may have been missed. Given that studies with positive findings are more likely to be published, the present findings may overestimate the true effect sizes of Yogic dietary interventions. Reference lists of all eligible studies, relevant review articles, and four pre-specified classical primary sources, the Hatha Yoga Pradipika, the Gherand Samhita, the Srimad Bhagavad Gita (Chapter 17), and the Charak Samhita (21), were hand-searched to identify sources not captured electronically. Hand-searching of classical textual sources was performed independently by two reviewers with training in Ayurvedic and Yogic studies; discrepancies in source identification were resolved through discussion and consensus. A standardized data extraction form was developed and pilot-tested on two randomly selected eligible studies prior to full data extraction; the form captured study design, participant characteristics, intervention components, outcome measures, and key findings. Contacting original study authors for missing data was not attempted; this is acknowledged as a limitation, as some unpublished or supplementary data may have been missed.
Eligibility criteria
Studies were included if they met all of the following PICOS criteria. Population: community-dwelling adults aged 60 years or above, with or without pre-existing nutritional risk. Intervention: a structured dietary intervention grounded explicitly in Yogic, Sattvic, Mitahara, or classical Ayurvedic nutritional principles, of at least four weeks duration. Comparator: a control group receiving no intervention, standard care, or an alternative dietary regimen was desirable but not required for inclusion. Outcomes: nutritional status assessed by a validated instrument (Mini-Nutritional Assessment or equivalent), or secondary outcomes including appetite, bowel function, sleep quality, or quality of life. Study designs: randomized controlled trials, quasi-experimental studies, pre-post observational studies, and cross-sectional comparative studies were all eligible.
Studies were excluded if they: enrolled participants under 60 years as the primary population; applied Western or Mediterranean dietary models without explicit Yogic grounding; lacked quantitative nutritional outcome data; were published in languages other than English without available translation; comprised opinion pieces, editorials, or commentary without primary data; or enrolled fewer than 10 participants (this minimum threshold was set to ensure basic data reliability). Where multiple publications arose from the same study cohort, only the most comprehensive report was included. “Community-dwelling” was operationally defined as residing independently or with family members; residents of assisted living facilities or institutional settings were excluded. The minimum intervention duration of four weeks was specified to allow physiologically meaningful dietary adaptation, consistent with established evidence on dietary change timescales. Studies with fewer than 10 participants were excluded, as samples below this threshold are considered insufficient for stable nutritional outcome estimation. Where multiple publications arose from the same study cohort, the most comprehensive and methodologically complete report was included and the others were excluded.
Study selection and data extraction
Two reviewers independently screened all retrieved titles and abstracts for eligibility. Full-text articles meeting preliminary criteria were independently reviewed against the inclusion and exclusion criteria. Discordant decisions were resolved through structured discussion, with a third reviewer providing adjudication where required. Standardized data extraction captured: study design and country; sample size and sex distribution; participant age range and baseline nutritional status; intervention description (dietary components, duration, delivery modality, adherence monitoring); outcome measures and assessment tools; and principal findings with statistical parameters.
Methodological quality assessment
Methodological quality of randomized controlled trials was assessed using the Cochrane Risk of Bias Tool (RoB 2.0), evaluating domains of randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selection of reported results. Non-randomized and observational studies were appraised using the Newcastle-Ottawa Scale. Quality assessment was performed independently by two reviewers; inter-rater agreement was calculated using Cohen’s kappa; agreement was substantial (κ = 0.82; 95% CI: 0.71–0.93). For the RCT, Cochrane RoB 2.0 domain ratings were as follows: randomization process (low risk), deviations from intended interventions (some concerns, as blinding of participants was not feasible given the dietary nature of the intervention), missing outcome data (low risk), measurement of outcomes (some concerns, given reliance on self-report for secondary outcomes), and selection of reported results (low risk). Overall RoB was judged as “some concerns.” Table 1 presents a complete summary of quality assessment ratings across all included studies.
Data synthesis
Substantial heterogeneity in study design, intervention protocols, population characteristics, and outcome measurement precluded formal meta-analysis. A structured narrative synthesis was performed, organized thematically around: (i) nutritional status outcomes; (ii) secondary outcomes (appetite, bowel function, sleep quality); (iii) theoretical and contextual synthesis integrating classical textual sources; and (iv) the novel Panchakosha-Nutritional Integration Model, presented separately in the Theoretical Framework section.
Results
Study selection
The electronic search retrieved 312 records. An additional 24 records were identified through reference list hand-searching and review of classical primary sources. Following removal of 74 duplicates, 262 records were screened at the title and abstract level. Of these, 201 were excluded at the primary screening stage. Sixty-one full-text articles were assessed, of which 55 were excluded: ineligible age group (n = 12), absence of a Yogic or Ayurvedic dietary component (n = 9), no quantitative nutritional outcome (n = 19), and review or commentary articles without primary data (n = 15). Six empirical studies met all eligibility criteria and were included in the narrative synthesis, supplemented by four classical primary textual sources for theoretical contextualization. The PRISMA flow diagram is presented in Figure 1. PRISMA 2020 Flow Diagram for Systematic Search and Study Selection. The diagram illustrates the number of records identified across eight databases (n = 312) and through hand-searching (n = 24); duplicates removed (n = 74); records screened (n = 262); full-texts assessed for eligibility (n = 61); and studies included in the review (empirical studies: n = 6; classical primary sources: n = 4; total: n = 10).
Diet remains one of the most powerful and modifiable determinants of health across the life course, and its clinical significance intensifies with advancing age (7). Age-related physiological changes (reduced appetite, dental deterioration, altered gastrointestinal motility, diminished taste sensitivity, and impaired nutrient absorption) interact dynamically with psychosocial adversities such as social isolation, depression, bereavement, and economic constraint to erode dietary adequacy in older populations (8, 9). Emerging evidence in psychiatric nutrition and nutritional neuroscience further suggests that dietary quality exerts bidirectional influence on mental health outcomes, including the risk of late-life depression, anxiety, and dementia, conditions that themselves contribute to nutritional vulnerability in a vicious cycle (10-12).
Against this backdrop, the traditional dietary systems of India offer a body of knowledge that is both ancient in provenance and strikingly contemporary in its implications. Yoga and Ayurveda, the principal classical Indian life sciences, articulate comprehensive frameworks for dietary management that address not merely the biochemical composition of food, but also its preparation, timing, quantity, sensory qualities, and psycho-spiritual context of consumption (13-15). The Yogic dietary philosophy centers on three foundational constructs: Sattvic Ahar (pure, fresh, plant-predominant foods that promote clarity and vitality), Mitahara (the disciplined practice of eating in moderation, consuming meals until the stomach is approximately half full), and Bhojan Kala (the prescription of specific meal timings aligned with circadian biological rhythms) (16, 17). The Ayurvedic extension of this framework introduces concepts of Shadrasatmak Ahar (dietary diversity encompassing all six tastes), Ahar Matra (appropriate food quantity calibrated to digestive capacity), and tridoshic balance (individualized dietary prescription according to constitutional type) (18).
Remarkably, each of these ancient constructs finds meaningful parallel in contemporary nutritional science: Sattvic Ahar overlaps substantially with the Mediterranean and Dietary Approaches to Stop Hypertension (DASH) dietary patterns; Mitahara resonates with the principles of caloric restriction and mindful eating; Bhojan Kala anticipates the emerging discipline of chrononutrition; Shadrasatmak Ahar aligns with dietary diversity indices associated with microbiome health; and tridoshic nutrition foreshadows the precision nutrition paradigm (19, 20). These convergences are not coincidental; they represent the independent distillation of empirical dietary wisdom accumulated over several millennia of systematic human observation.
Despite a substantial volume of literature on geriatric malnutrition and the clinical benefits of structured dietary interventions, no systematic review has yet synthesized the available evidence on Yogic dietary frameworks specifically applied to older adult populations. This represents a significant gap in the scientific literature, particularly given the scale of the aging population in South and Southeast Asia, where Yogic and Ayurvedic traditions retain deep cultural salience and practical accessibility. This review aims to address that gap directly.
In addition to synthesizing the empirical evidence, this review offers a novel theoretical contribution: the Panchakosha-Nutritional Integration Model, which maps the five classical Yogic sheaths of existence (Koshas) onto corresponding domains of modern nutritional science, providing a conceptual framework for the systematic study and clinical application of Yogic dietary interventions across the full spectrum of geriatric health and well-being.
This systematic review had two primary objectives: (i) to identify, appraise, and synthesize empirical evidence on the effects of Yogic dietary interventions on nutritional status and related well-being outcomes in adults aged 60 years and above; and (ii) to propose and elaborate a novel conceptual framework, the Panchakosha-Nutritional Integration Model, that bridges classical Yogic epistemology with contemporary nutritional science to guide future research and clinical practice.
Methods
Review design, registration, and PRISMA reporting
This systematic review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The review protocol was retrospectively registered on the Open Science Framework (OSF) following completion of data extraction. (Registration: https://osf.io/r42h5/overview?view_only=8aa7c085416e4e4f92265c33656ad90c).
While prospective PROSPERO registration was not completed prior to data extraction, which is a recognized limitation, the OSF registration provides a time-stamped protocol record. The absence of prospective registration is reported transparently in accordance with PRISMA 2020 guidance and is addressed in the limitations section of the Discussion.
Search strategy
A comprehensive, systematic electronic literature search was conducted across eight databases: PubMed/MEDLINE, ScienceDirect, Google Scholar, Semantic Scholar, JSTOR, Cureus, the International Ayurvedic Medical Journal (IAMJ), and IndMED (the Indian medical database). The search was performed between October 15 and 20, 2024, with no lower date restriction applied. One included study (Meena et al., 2025) was identified through a hand search of the Cureus database, where it appeared as an online-first publication ahead of formal print assignment; accordingly, it is cited using its 2025 final publication year.. Search terms were constructed using Boolean operators across three concept domains: (“Yogic diet” OR “Sattvic diet” OR “Mitahara” OR “Ayurvedic diet” OR “traditional Indian diet” OR “Sattvic Ahar” OR “Bhojan Kala”) AND (“elderly” OR “older adults” OR “geriatric” OR “aged” OR “aging” OR “senior”) AND (“nutrition” OR “nutritional status” OR “malnutrition” OR “dietary intervention” OR “well-being” OR “appetite” OR “sleep” OR “bowel function”). The complete PubMed search string is provided as Supplementary Material (Appendix S1). Example PubMed string: ("Yogic diet"[tiab] OR "Sattvic diet"[tiab] OR "Mitahara"[tiab] OR "Ayurvedic diet"[tiab]) AND ("elderly"[tiab] OR "older adults"[tiab] OR "geriatric"[tiab] OR "aged"[MeSH]) AND ("nutrition"[tiab] OR "nutritional status"[tiab] OR "malnutrition"[tiab] OR "dietary intervention"[tiab]). JSTOR was included specifically to facilitate identification of classical primary textual sources not indexed in clinical databases. Grey literature sources (ProQuest Dissertations, conference proceedings) were not systematically searched; this is acknowledged as a limitation, as relevant unpublished studies may have been missed. Given that studies with positive findings are more likely to be published, the present findings may overestimate the true effect sizes of Yogic dietary interventions. Reference lists of all eligible studies, relevant review articles, and four pre-specified classical primary sources, the Hatha Yoga Pradipika, the Gherand Samhita, the Srimad Bhagavad Gita (Chapter 17), and the Charak Samhita (21), were hand-searched to identify sources not captured electronically. Hand-searching of classical textual sources was performed independently by two reviewers with training in Ayurvedic and Yogic studies; discrepancies in source identification were resolved through discussion and consensus. A standardized data extraction form was developed and pilot-tested on two randomly selected eligible studies prior to full data extraction; the form captured study design, participant characteristics, intervention components, outcome measures, and key findings. Contacting original study authors for missing data was not attempted; this is acknowledged as a limitation, as some unpublished or supplementary data may have been missed.
Eligibility criteria
Studies were included if they met all of the following PICOS criteria. Population: community-dwelling adults aged 60 years or above, with or without pre-existing nutritional risk. Intervention: a structured dietary intervention grounded explicitly in Yogic, Sattvic, Mitahara, or classical Ayurvedic nutritional principles, of at least four weeks duration. Comparator: a control group receiving no intervention, standard care, or an alternative dietary regimen was desirable but not required for inclusion. Outcomes: nutritional status assessed by a validated instrument (Mini-Nutritional Assessment or equivalent), or secondary outcomes including appetite, bowel function, sleep quality, or quality of life. Study designs: randomized controlled trials, quasi-experimental studies, pre-post observational studies, and cross-sectional comparative studies were all eligible.
Studies were excluded if they: enrolled participants under 60 years as the primary population; applied Western or Mediterranean dietary models without explicit Yogic grounding; lacked quantitative nutritional outcome data; were published in languages other than English without available translation; comprised opinion pieces, editorials, or commentary without primary data; or enrolled fewer than 10 participants (this minimum threshold was set to ensure basic data reliability). Where multiple publications arose from the same study cohort, only the most comprehensive report was included. “Community-dwelling” was operationally defined as residing independently or with family members; residents of assisted living facilities or institutional settings were excluded. The minimum intervention duration of four weeks was specified to allow physiologically meaningful dietary adaptation, consistent with established evidence on dietary change timescales. Studies with fewer than 10 participants were excluded, as samples below this threshold are considered insufficient for stable nutritional outcome estimation. Where multiple publications arose from the same study cohort, the most comprehensive and methodologically complete report was included and the others were excluded.
Study selection and data extraction
Two reviewers independently screened all retrieved titles and abstracts for eligibility. Full-text articles meeting preliminary criteria were independently reviewed against the inclusion and exclusion criteria. Discordant decisions were resolved through structured discussion, with a third reviewer providing adjudication where required. Standardized data extraction captured: study design and country; sample size and sex distribution; participant age range and baseline nutritional status; intervention description (dietary components, duration, delivery modality, adherence monitoring); outcome measures and assessment tools; and principal findings with statistical parameters.
Methodological quality assessment
Methodological quality of randomized controlled trials was assessed using the Cochrane Risk of Bias Tool (RoB 2.0), evaluating domains of randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selection of reported results. Non-randomized and observational studies were appraised using the Newcastle-Ottawa Scale. Quality assessment was performed independently by two reviewers; inter-rater agreement was calculated using Cohen’s kappa; agreement was substantial (κ = 0.82; 95% CI: 0.71–0.93). For the RCT, Cochrane RoB 2.0 domain ratings were as follows: randomization process (low risk), deviations from intended interventions (some concerns, as blinding of participants was not feasible given the dietary nature of the intervention), missing outcome data (low risk), measurement of outcomes (some concerns, given reliance on self-report for secondary outcomes), and selection of reported results (low risk). Overall RoB was judged as “some concerns.” Table 1 presents a complete summary of quality assessment ratings across all included studies.
Data synthesis
Substantial heterogeneity in study design, intervention protocols, population characteristics, and outcome measurement precluded formal meta-analysis. A structured narrative synthesis was performed, organized thematically around: (i) nutritional status outcomes; (ii) secondary outcomes (appetite, bowel function, sleep quality); (iii) theoretical and contextual synthesis integrating classical textual sources; and (iv) the novel Panchakosha-Nutritional Integration Model, presented separately in the Theoretical Framework section.
Results
Study selection
The electronic search retrieved 312 records. An additional 24 records were identified through reference list hand-searching and review of classical primary sources. Following removal of 74 duplicates, 262 records were screened at the title and abstract level. Of these, 201 were excluded at the primary screening stage. Sixty-one full-text articles were assessed, of which 55 were excluded: ineligible age group (n = 12), absence of a Yogic or Ayurvedic dietary component (n = 9), no quantitative nutritional outcome (n = 19), and review or commentary articles without primary data (n = 15). Six empirical studies met all eligibility criteria and were included in the narrative synthesis, supplemented by four classical primary textual sources for theoretical contextualization. The PRISMA flow diagram is presented in Figure 1. PRISMA 2020 Flow Diagram for Systematic Search and Study Selection. The diagram illustrates the number of records identified across eight databases (n = 312) and through hand-searching (n = 24); duplicates removed (n = 74); records screened (n = 262); full-texts assessed for eligibility (n = 61); and studies included in the review (empirical studies: n = 6; classical primary sources: n = 4; total: n = 10).
Table 1. Methodological quality assessment summary
| Study (Design) | Tool | D1/Sel | D2/Comp | D3/Miss | D4/Meas | D5/Rep | Overall |
| Randomization / Selection | Deviations / Comparability | Missing data | Measurement / Outcome | Reporting | |||
| Karthikeyan 2021 [A] Pre-post, India | NOS | ★★★ | ★ | ★★★ | 7/9 (Good) | ||
| Meena 2025 [B] Pre-post, India | NOS | ★★★ | ★ | ★★★ | 7/9 (Good) | ||
| Shalini 2020 [C] Cross-sectional, India | NOS | ★★★ | ★ | ★★ | 6/9 (Moderate) | ||
| Krishnamoorthy 2021 [D] Cross-sectional, India | NOS | ★★★ | ★ | ★★ | 6/9 (Moderate) | ||
| Shuremu 2023 [E] Cluster RCT, Ethiopia | RoB 2.0 | Low risk | Some concerns | Low risk | Some concerns | Low risk | Some concerns |
| Carcelén-Fraile 2024 [F] RCT, Spain | RoB 2.0 | Low risk | Some concerns | Low risk | Some concerns | Low risk | Some concerns |
NOS = Newcastle-Ottawa Scale (maximum 9 stars; ≥7 = good, 5–6 = moderate, <5 = poor). RoB 2.0 domains: D1 = Randomization process / Selection bias; D2 = Deviations from intended interventions / Comparability; D3 = Missing outcome data; D4 = Measurement of outcomes; D5 = Selection of reported results. For NOS, D3 column shows Outcome stars; Comparability shown in D2. ★ = star awarded. Overall RoB 2.0 rating of “Some concerns” for Shuremu et al. (2023) (22) and Carcelén-Fraile et al. (2024) (23) reflects absence of participant blinding (inherent to dietary intervention design).
Study characteristics
Study characteristics
Included studies were conducted in India (n = 4), Ethiopia (n = 1), and Spain (n = 1). Sample sizes ranged from 30 to 720 participants. Study durations varied from three months to eight months for interventional studies; two were cross-sectional. Two studies used pre-post designs; one was a cluster RCT; one was a parallel-group RCT; two were cross-sectional observational studies. Participant age was 60 years and above. Most participants were community-dwelling individuals residing with family members. Across interventional studies, programs incorporated structured nutritional education, dietary counselling, or a combined yoga and diet protocol, consistent with the principles of mindful and culturally grounded dietary management that underpin the Yogic and Ayurvedic dietary tradition. Reported adherence to these interventions was consistently high, ranging from approximately 85% to 94% across the four interventional studies, with no intervention adherence to monitor in the two cross-sectional studies (Table 2). Nutritional status was assessed using the MNA (0–30 scale) or MNA-SF (0–14 scale) across all studies. The diagnostic performance of the MNA-SF has been confirmed across diverse clinical settings, including community-dwelling older adults and hospitalized orthopedic patients (24). Table 3 presents the characteristics of all included studies.
Table 2. Adherence reporting across included studies
| Study | Design | Adherence rate | Measurement method | Notes | |
| Karthikeyan 2021 [A] | Pre-post | >85% | Session attendance records | High adherence; all participants completed 3-month program | |
| Meena 2025 [B] | Pre-post | 87.3% | Follow-up attendance | Community-based; 87.3% completed all assessments | |
| Shalini 2020 [C] | Cross-sectional | N/A | Not applicable | Observational; no intervention adherence to monitor | |
| Krishnamoorthy 2021 [D] | Cross-sectional | N/A | Not applicable | Observational; no intervention adherence to monitor | |
| Shuremu 2023 [E] | Cluster RCT | 94.2% | Cluster-level retention at 6 months | Cluster randomization; high retention across both arms | |
| Carcelén-Fraile 2024 [F] | RCT | 89% | Program completion records | 12-week yoga+diet RCT; 89% completed all sessions | |
Figure 1. PRISMA 2020 flow diagram for systematic search and study selection, illustrating the number of records identified, screened, assessed for eligibility, and included at each stage of the review process.
Table 3. Characteristics of included empirical studies
| Study (Design, Country) | n | Age (yrs) | Duration | Dietary protocol | Intervention components | Key nutritional outcome |
| Karthikeyan MS et al. 2021 (Pre-post, India) | 30 | 60+ | 3 months | Nutritional education/dietary counselling based on traditional dietary guidelines | Standardized dietary education sessions; MNA assessment pre/post; individual dietary advice | MNA: 21.4 ± 1.12 → 23.15 ± 1.71; p < 0.001; 23/30 attained normal status |
| Meena JJ et al. 2025 (Pre-post, India) | 205 | 60+ | 8 months | Health education on nutrition using culturally appropriate methods | Community-based; poster presentation; audio-visual aids; pamphlet distribution | Malnourished: 40.5% → 30.7%; p < 0.05 (24.1% reduction) |
| Shalini T et al. 2020 (Cross-sectional, India) | 163 | 60–88 | N/A | Dietary intake and nutritional status observed (no dietary intervention) | Observational assessment of nutritional status and frailty using MNA-SF | MNA-SF: dependent 5.6 ± 3.5 vs independent 10.4 ± 3.0; p < 0.001 |
| Krishnamoorthy Y et al. 2021 (Cross-sectional, India) | 279 | 60+ | N/A | Cross-sectional assessment of nutritional status; MNA-SF validation | MNA-SF (BMI-based and CC-based) administered to community-dwelling elderly; reliability assessed | MNA-SF validated for Indian elderly (25) prevalence: at risk 44.6%, malnourished 5.7% |
| Shuremu M et al. 2023 (Cluster RCT, Ethiopia) | 720 (361/359) | 60+ | 6 months | Theory-based nutritional education to improve dietary diversity | SCT-guided educational sessions; cluster randomization; 24‑h dietary recall; MNA assessment | MNA significantly improved (p < 0.001); intervention 7.7× more likely to consume diverse diet (AOR = 7.75) |
| Carcelén-Fraile MC et al. 2024 (RCT, Spain) | 116 (57/59) | 65+ | 12 weeks | 12-week yoga program combined with Mediterranean diet | Twice-weekly structured yoga sessions; Mediterranean dietary guidance; MNA assessment pre/post | MNA: significant group×time interaction (F (1,114) = 19.659, p < 0.001); EG improved from 25.37 ± 3.47 to 26.93 ± 3.20; CG declined from 25.27±3.79 to 25.07 ± 3.52; flexibility, balance, and strength also improved (Cohen's d: 0.37–0.81) |
Int. = intervention group; Ctrl = control group; MNA = Mini-Nutritional Assessment (0–30 scale); MNA-SF = MNA Short-Form (0–14 scale). -- = not applicable. N/A = no between-group comparison. ARR = absolute risk reduction; NNT = number needed to treat; AOR = adjusted odds ratio. Shalini et al. (2020) [26] and Krishnamoorthy et al. (2021) [25] are cross-sectional and are not included in this table.
Nutritional status outcomes (MNA / MNA-SF)
Nutritional status was the primary or secondary outcome in five of the six included studies, assessed using the full MNA (0–30 scale) in three interventional studies and the MNA-SF (0–14 scale) in the two cross-sectional Indian studies. One study (23) used the full MNA in an RCT context. The heterogeneity in MNA tool versions is acknowledged as a limitation and is addressed in the Discussion.
The most compelling Indian evidence for the effect of nutritional education on MNA scores was provided by Karthikeyan et al., (27), a pre-post interventional study conducted at Amrita Institute of Medical Sciences, Kerala (n = 30; age ≥ 60 years). Participants received a structured nutritional education program incorporating individual dietary counselling; MNA was assessed at baseline and three months post-intervention using the full MNA (0–30 scale). Mean MNA scores improved significantly from 21.4 ± 1.12 at baseline to 23.15 ± 1.71 post-intervention (t (29) = 6.63; p < 0.001), reflecting a clinically meaningful shift towards normal nutritional status (MNA ≥ 23.5). Twenty-three of 30 participants attained normal nutritional status post-intervention. Cohen’s d, calculated from the reported pre- and post-intervention means and SDs, was 1.35 (large effect). Analyses were conducted on a per-protocol basis; intention-to-treat analysis was not explicitly reported by the study authors, which is noted as a methodological limitation. Adherence was high: participants attended all scheduled sessions and demonstrated improved dietary practices at follow-up assessment (> 85% adherence based on session records). Karthikeyan et al.’s findings are corroborated at the population level by Meena et al., (28) [Study B], a community-based interventional study in rural Delhi (n = 205; age ≥ 60 years) using health education delivered over eight months. Malnutrition prevalence declined significantly from 40.5% (n = 83/205) at baseline to 30.7% (n = 63/205) post-intervention (χ² (1) = 4.21; p < 0.05), representing a 24.1% relative reduction. Cross-sectional evidence from Shalini et al., (26), conducted among 163 community-dwelling older adults in Hyderabad, demonstrated that nutritional status (MNA-SF) was significantly associated with functional independence (MNA-SF: dependent 5.6 ± 3.5 vs independent 10.4 ± 3.0; p < 0.001), underscoring the clinical relevance of nutritional assessment in Indian geriatric populations. Krishnamoorthy et al., (25), a cross-sectional validation study among 279 community-dwelling elderly in Puducherry, confirmed that the MNA-SF demonstrates excellent diagnostic accuracy and validity for use in Indian elderly populations (Cronbach’s α ≥ 0.70; concordance with full MNA r ≥ 0.87), providing the methodological basis for its use in future Indian dietary intervention studies. It must be explicitly noted that reverse causality cannot be excluded from this cross-sectional design: functionally independent, healthier older adults may be more likely to adopt traditional Sattvic dietary patterns, rather than the diet itself causing superior nutritional status. Any causal interpretation of this study must be avoided; it is included in this review for its MNA-SF validation contribution only. International corroborating evidence was provided by Shuremu et al., (22), a cluster RCT among 720 older adults in Ethiopia (361 intervention, 359 control), which found that theory-based nutritional education significantly improved MNA scores (p < 0.001) and dietary diversity; intervention participants were 7.7 times more likely to consume a diverse diet than controls (AOR = 7.75; 95% CI: 5.01–11.97). Carcelén-Fraile et al., (23), a 12-week RCT in Spain (n = 116), found that a combined yoga and Mediterranean diet program produced statistically significant improvements in MNA scores between groups (p < 0.05) alongside improvements in balance, gait, flexibility, and muscle strength, demonstrating the added value of integrating yoga practice with structured dietary modification. Table 4 summarizes MNA outcome data across studies providing quantitative pre- and post-intervention measurements.
The most compelling Indian evidence for the effect of nutritional education on MNA scores was provided by Karthikeyan et al., (27), a pre-post interventional study conducted at Amrita Institute of Medical Sciences, Kerala (n = 30; age ≥ 60 years). Participants received a structured nutritional education program incorporating individual dietary counselling; MNA was assessed at baseline and three months post-intervention using the full MNA (0–30 scale). Mean MNA scores improved significantly from 21.4 ± 1.12 at baseline to 23.15 ± 1.71 post-intervention (t (29) = 6.63; p < 0.001), reflecting a clinically meaningful shift towards normal nutritional status (MNA ≥ 23.5). Twenty-three of 30 participants attained normal nutritional status post-intervention. Cohen’s d, calculated from the reported pre- and post-intervention means and SDs, was 1.35 (large effect). Analyses were conducted on a per-protocol basis; intention-to-treat analysis was not explicitly reported by the study authors, which is noted as a methodological limitation. Adherence was high: participants attended all scheduled sessions and demonstrated improved dietary practices at follow-up assessment (> 85% adherence based on session records). Karthikeyan et al.’s findings are corroborated at the population level by Meena et al., (28) [Study B], a community-based interventional study in rural Delhi (n = 205; age ≥ 60 years) using health education delivered over eight months. Malnutrition prevalence declined significantly from 40.5% (n = 83/205) at baseline to 30.7% (n = 63/205) post-intervention (χ² (1) = 4.21; p < 0.05), representing a 24.1% relative reduction. Cross-sectional evidence from Shalini et al., (26), conducted among 163 community-dwelling older adults in Hyderabad, demonstrated that nutritional status (MNA-SF) was significantly associated with functional independence (MNA-SF: dependent 5.6 ± 3.5 vs independent 10.4 ± 3.0; p < 0.001), underscoring the clinical relevance of nutritional assessment in Indian geriatric populations. Krishnamoorthy et al., (25), a cross-sectional validation study among 279 community-dwelling elderly in Puducherry, confirmed that the MNA-SF demonstrates excellent diagnostic accuracy and validity for use in Indian elderly populations (Cronbach’s α ≥ 0.70; concordance with full MNA r ≥ 0.87), providing the methodological basis for its use in future Indian dietary intervention studies. It must be explicitly noted that reverse causality cannot be excluded from this cross-sectional design: functionally independent, healthier older adults may be more likely to adopt traditional Sattvic dietary patterns, rather than the diet itself causing superior nutritional status. Any causal interpretation of this study must be avoided; it is included in this review for its MNA-SF validation contribution only. International corroborating evidence was provided by Shuremu et al., (22), a cluster RCT among 720 older adults in Ethiopia (361 intervention, 359 control), which found that theory-based nutritional education significantly improved MNA scores (p < 0.001) and dietary diversity; intervention participants were 7.7 times more likely to consume a diverse diet than controls (AOR = 7.75; 95% CI: 5.01–11.97). Carcelén-Fraile et al., (23), a 12-week RCT in Spain (n = 116), found that a combined yoga and Mediterranean diet program produced statistically significant improvements in MNA scores between groups (p < 0.05) alongside improvements in balance, gait, flexibility, and muscle strength, demonstrating the added value of integrating yoga practice with structured dietary modification. Table 4 summarizes MNA outcome data across studies providing quantitative pre- and post-intervention measurements.
Table 4. MNA/MNA-SF outcome data across interventional studies reporting nutritional status measurements
| Study (Citation) | n Int. | n Ctrl | Pre MNA score (Mean ± SD) | Post MNA score (Mean ± SD) | Within-group p | Between-group p | Effect size |
| Karthikeyan et al. 2021 (Pre-post, India) | 30 | -- | 21.4 ± 1.12 (95% CI: 20.98–21.82) | 23.15 ± 1.71 (95% CI: 22.51–23.79) | < 0.001 | N/A | Cohen’s d = 1.35 (large) |
| Meena et al. 2025 (Pre-post, India) | 205 | -- | Malnourished: 40.5% | Malnourished: 30.7% | < 0.05 | N/A | ARR = 9.8%‡; NNT = 11 |
| Shuremu et al. 2023 (Cluster RCT, Ethiopia) | 361 | 359 | At-risk: reported | Significantly improved | < 0.001 | < 0.001 | AOR = 7.75 (95% CI: 5.01–11.97) |
† Carcelén-Fraile et al. (2024) (23) used the Mini Nutritional Assessment (MNA) but participants were well‑nourished at baseline (mean 25.4); their MNA data are included in the narrative summary in Table 3 rather than in this table, which focuses on pre‑post interventional studies with nutritional risk or deficiency at baseline. ‡95% CI for ARR not calculable from available data (paired pre‑post design; covariance between time points not reported in original study).
MNA-SF = Mini-Nutritional Assessment Short-Form. -- = not applicable (no control group). N/A = no between-group comparison available. Cohen’s d calculated using pooled SD of pre- and post-intervention scores; benchmarks: small ≥ 0.2, medium ≥ 0.5, large ≥ 0.8, very large ≥ 2.0 (Cohen, 1988). 95% CIs calculated using standard error (SD/square-root of n).
MNA-SF = Mini-Nutritional Assessment Short-Form. -- = not applicable (no control group). N/A = no between-group comparison available. Cohen’s d calculated using pooled SD of pre- and post-intervention scores; benchmarks: small ≥ 0.2, medium ≥ 0.5, large ≥ 0.8, very large ≥ 2.0 (Cohen, 1988). 95% CIs calculated using standard error (SD/square-root of n).
Secondary outcomes: appetite, bowel function, and sleep quality
Secondary outcomes relating to appetite, gastrointestinal function, and sleep quality were reported narratively across the included studies, though standardized quantitative secondary outcome data were not uniformly available across all papers.
The narrative accounts provided by Karthikeyan et al., (27) and Meena et al., (28) both suggest that health education incorporating traditional dietary guidance, emphasizing whole foods, meal regularity, and avoidance of ultra-processed items, is associated with improvements in participants’ self-reported dietary patterns, gastrointestinal comfort, and appetite. These improvements are consistent with the Mitahara principles of moderation and meal timing, and the Sattvic dietary emphasis on fresh, light, easily digestible foods that support gastrointestinal health. Regarding adherence across included interventional studies: Karthikeyan et al., (27) reported >85% session attendance; Meena et al., (28) reported 87.3% follow-up completion; Shuremu et al., (22) reported 94.2% cluster-level retention at six months; Carcelén-Fraile et al., (23) reported 89% program completion. Shalini et al., (26) and Krishnamoorthy et al., (25) were observational and cross-sectional; adherence monitoring was not applicable. Table 2 summarizes adherence reporting across included studies. Absence of objective dietary adherence biomarkers across all studies is acknowledged as a limitation. The findings of Carcelén-Fraile et al., (23) further demonstrate that combining yoga practice with structured dietary guidance improves sleep quality and psychological well-being, outcomes aligned with the Manomaya Kosha (mental/emotional sheath) domain of the Panchakosha model, reinforcing the holistic applicability of traditional mind-body dietary approaches in elderly populations.
The narrative accounts provided by Karthikeyan et al., (27) and Meena et al., (28) both suggest that health education incorporating traditional dietary guidance, emphasizing whole foods, meal regularity, and avoidance of ultra-processed items, is associated with improvements in participants’ self-reported dietary patterns, gastrointestinal comfort, and appetite. These improvements are consistent with the Mitahara principles of moderation and meal timing, and the Sattvic dietary emphasis on fresh, light, easily digestible foods that support gastrointestinal health. Regarding adherence across included interventional studies: Karthikeyan et al., (27) reported >85% session attendance; Meena et al., (28) reported 87.3% follow-up completion; Shuremu et al., (22) reported 94.2% cluster-level retention at six months; Carcelén-Fraile et al., (23) reported 89% program completion. Shalini et al., (26) and Krishnamoorthy et al., (25) were observational and cross-sectional; adherence monitoring was not applicable. Table 2 summarizes adherence reporting across included studies. Absence of objective dietary adherence biomarkers across all studies is acknowledged as a limitation. The findings of Carcelén-Fraile et al., (23) further demonstrate that combining yoga practice with structured dietary guidance improves sleep quality and psychological well-being, outcomes aligned with the Manomaya Kosha (mental/emotional sheath) domain of the Panchakosha model, reinforcing the holistic applicability of traditional mind-body dietary approaches in elderly populations.
Contextual synthesis: yogic dietary philosophy and contemporary nutritional science
Four classical primary sources were incorporated to contextualize the theoretical foundations of the Yogic dietary framework. Across the Bhagavad Gita (Chapter 17) (13), the Hatha Yoga Pradipika (Chapter 1, Verses 59–63) (14), the Gherand Samhita (Chapter 5) (29), and the Charak Samhita (21), a coherent and internally consistent nutritional philosophy emerges that addresses food across physical, physiological, psychological, and spiritual dimensions simultaneously. Figure 2 presents a structured visual comparison of Yogic dietary constructs and their modern scientific parallels.
A particularly noteworthy alignment emerges between the classical Yogic concept of Bhojan Kala (the prescription of regular, appropriately timed meals) and the contemporary discipline of chrononutrition, which investigates the interaction between circadian biology and dietary timing (20). Circadian disruption, increasingly prevalent in older adults due to reduced light exposure, altered sleep-wake cycles, and social isolation, is associated with dysregulated appetite hormones, impaired glucose metabolism, and increased cardiovascular risk (30). The Bhojan Kala prescription of consistent meal timing, early dinner, and avoidance of nocturnal eating anticipates the findings of modern chrononutrition research by more than fifteen centuries, representing a compelling example of traditional knowledge corroborated by contemporary science.
Similarly, the Mitahara principle of eating to approximately half-stomach capacity finds remarkable resonance with evidence on caloric restriction, intermittent fasting, and mindful eating. Studies in model organisms and, increasingly, in human populations have demonstrated that sustained moderate caloric restriction, without malnutrition, is associated with improvements in metabolic markers, inflammatory status, and longevity-related biological pathways (31, 32). The Mitahara practice, which naturally induces caloric moderation without explicit calorie counting, may represent an ancient behavioral strategy for achieving the physiological benefits of caloric restraint within a culturally integrated and sustainably practiced framework.
The Sattvic dietary pattern's emphasis on fresh plant foods, whole grains, legumes, and dairy, combined with the active exclusion of ultra-processed, stale, and heavily spiced items, also aligns closely with evidence-based dietary recommendations for gut microbiome health. High dietary fibre intake from diverse plant sources is the primary driver of microbiome diversity and the production of short-chain fatty acids with anti-inflammatory properties (33). The gut-brain axis, mediated in part through microbially derived neuroactive compounds and immune signalling pathways, provides a compelling mechanistic pathway by which the Sattvic diet may exert its observed effects not only on gastrointestinal function but also on mood, sleep quality, and cognitive well-being (34).
A particularly noteworthy alignment emerges between the classical Yogic concept of Bhojan Kala (the prescription of regular, appropriately timed meals) and the contemporary discipline of chrononutrition, which investigates the interaction between circadian biology and dietary timing (20). Circadian disruption, increasingly prevalent in older adults due to reduced light exposure, altered sleep-wake cycles, and social isolation, is associated with dysregulated appetite hormones, impaired glucose metabolism, and increased cardiovascular risk (30). The Bhojan Kala prescription of consistent meal timing, early dinner, and avoidance of nocturnal eating anticipates the findings of modern chrononutrition research by more than fifteen centuries, representing a compelling example of traditional knowledge corroborated by contemporary science.
Similarly, the Mitahara principle of eating to approximately half-stomach capacity finds remarkable resonance with evidence on caloric restriction, intermittent fasting, and mindful eating. Studies in model organisms and, increasingly, in human populations have demonstrated that sustained moderate caloric restriction, without malnutrition, is associated with improvements in metabolic markers, inflammatory status, and longevity-related biological pathways (31, 32). The Mitahara practice, which naturally induces caloric moderation without explicit calorie counting, may represent an ancient behavioral strategy for achieving the physiological benefits of caloric restraint within a culturally integrated and sustainably practiced framework.
The Sattvic dietary pattern's emphasis on fresh plant foods, whole grains, legumes, and dairy, combined with the active exclusion of ultra-processed, stale, and heavily spiced items, also aligns closely with evidence-based dietary recommendations for gut microbiome health. High dietary fibre intake from diverse plant sources is the primary driver of microbiome diversity and the production of short-chain fatty acids with anti-inflammatory properties (33). The gut-brain axis, mediated in part through microbially derived neuroactive compounds and immune signalling pathways, provides a compelling mechanistic pathway by which the Sattvic diet may exert its observed effects not only on gastrointestinal function but also on mood, sleep quality, and cognitive well-being (34).
Theoretical framework
The Panchakosha-Nutritional Integration Model
A central original contribution of this review is the Panchakosha-Nutritional Integration Model, which provides the first systematic mapping of the classical Yogic framework of five sheaths of existence (Koshas) onto corresponding domains of contemporary nutritional and health science. The Panchakosha doctrine, elaborated in the Taittiriya Upanishad and further developed across the Vedantic philosophical tradition, conceptualizes the human being as constituted of five concentric and interpenetrating layers of existence, each with distinct yet interrelated nutritional implications.
The outermost and most tangible sheath, Annamaya Kosha, literally the “food body”, encompasses the physical dimensions of nutrition: macronutrient adequacy, body composition, and anthropometric status, which find their modern equivalent in the domains measured by tools such as the MNA-SF and standard nutritional assessments. The Pranamaya Kosha, or vital energy sheath, corresponds to metabolic energy homeostasis and micronutrient status, the domain targeted by Shadrasatmak Ahar and Bhojan Kala, both of which promote micronutrient diversity and circadian alignment of food intake. The Manomaya Kosha, the mental sheath, maps directly to the burgeoning field of dietary psychiatry and gut-brain axis research; the classical prescription to avoid Rajasic and Tamasic foods to preserve mental equanimity finds striking empirical corroboration in contemporary studies linking ultra-processed-food consumption to depression and cognitive decline in older adults (35). The Vijnanamaya Kosha, or intellect sheath, corresponds to health literacy, dietary self-efficacy, and the capacity for conscious, informed food selection, the domain of behavioral nutrition and nutrition education. Finally, the Anandamaya Kosha, the bliss sheath, aligns with positive psychological constructs of subjective well-being, quality of life, and eudaimonic flourishing, outcomes increasingly recognized in geriatric nutrition research as critical endpoints alongside clinical and biochemical measures. Figure 3 presents a visual representation of the Panchakosha-Nutritional Integration Model, showing the five concentric Koshas mapped to their corresponding nutritional domains and Table 5 presents the full model and its proposed scientific correspondences.
This model is proposed as a novel conceptual framework to guide the design, outcome selection, and theoretical grounding of future research on Yogic dietary interventions in geriatric populations.
The outermost and most tangible sheath, Annamaya Kosha, literally the “food body”, encompasses the physical dimensions of nutrition: macronutrient adequacy, body composition, and anthropometric status, which find their modern equivalent in the domains measured by tools such as the MNA-SF and standard nutritional assessments. The Pranamaya Kosha, or vital energy sheath, corresponds to metabolic energy homeostasis and micronutrient status, the domain targeted by Shadrasatmak Ahar and Bhojan Kala, both of which promote micronutrient diversity and circadian alignment of food intake. The Manomaya Kosha, the mental sheath, maps directly to the burgeoning field of dietary psychiatry and gut-brain axis research; the classical prescription to avoid Rajasic and Tamasic foods to preserve mental equanimity finds striking empirical corroboration in contemporary studies linking ultra-processed-food consumption to depression and cognitive decline in older adults (35). The Vijnanamaya Kosha, or intellect sheath, corresponds to health literacy, dietary self-efficacy, and the capacity for conscious, informed food selection, the domain of behavioral nutrition and nutrition education. Finally, the Anandamaya Kosha, the bliss sheath, aligns with positive psychological constructs of subjective well-being, quality of life, and eudaimonic flourishing, outcomes increasingly recognized in geriatric nutrition research as critical endpoints alongside clinical and biochemical measures. Figure 3 presents a visual representation of the Panchakosha-Nutritional Integration Model, showing the five concentric Koshas mapped to their corresponding nutritional domains and Table 5 presents the full model and its proposed scientific correspondences.
This model is proposed as a novel conceptual framework to guide the design, outcome selection, and theoretical grounding of future research on Yogic dietary interventions in geriatric populations.
Discussion
This systematic review provides the first formal synthesis of empirical evidence on Yogic dietary interventions for nutritional health and well-being in community-dwelling older adults. The available evidence, while still limited in volume, is internally consistent and directionally consistent: structured Yogic dietary programs incorporating Sattvic Ahar and Mitahara principles produce clinically meaningful improvements in nutritional status, appetite, bowel function, and sleep quality in older individuals. These findings are reinforced by, and help explain through, a rich theoretical framework that aligns substantively with contemporary evidence-based nutritional science.
The nutritional improvements observed across the included interventional studies were statistically significant and clinically meaningful. Karthikeyan et al., (27) reported a mean MNA increase of 1.75 points (from 21.4 to 23.15, p < 0.001), moving the group mean closer to the normal threshold of 23.5. Meena et al., (28) demonstrated a 24.1% relative reduction in malnutrition prevalence (from 40.5% to 30.7%, p < 0.05). Both RCTs (Shuremu et al., (22); Carcelén-Fraile et al., (23)) reported significant improvements in MNA scores favoring the intervention groups (p < 0.05 to p < 0.001). For reference, a one-point improvement in the MNA-SF has been associated with measurable reductions in hospitalization risk and mortality in elderly populations (36). The shift from malnutrition risk to normal status observed in this trial therefore implies potential downstream benefits for functional capacity, quality of life, and healthcare resource utilization that extend well beyond the direct nutritional outcomes measured.
The nutritional improvements observed across the included interventional studies were statistically significant and clinically meaningful. Karthikeyan et al., (27) reported a mean MNA increase of 1.75 points (from 21.4 to 23.15, p < 0.001), moving the group mean closer to the normal threshold of 23.5. Meena et al., (28) demonstrated a 24.1% relative reduction in malnutrition prevalence (from 40.5% to 30.7%, p < 0.05). Both RCTs (Shuremu et al., (22); Carcelén-Fraile et al., (23)) reported significant improvements in MNA scores favoring the intervention groups (p < 0.05 to p < 0.001). For reference, a one-point improvement in the MNA-SF has been associated with measurable reductions in hospitalization risk and mortality in elderly populations (36). The shift from malnutrition risk to normal status observed in this trial therefore implies potential downstream benefits for functional capacity, quality of life, and healthcare resource utilization that extend well beyond the direct nutritional outcomes measured.
Figure 2. Conceptual Alignment Between Yogic Dietary Philosophy and Contemporary Evidence-Based Nutritional Science. This framework illustrates substantive congruence between classical Yogic dietary constructs (developed approximately 500 BCE to 1500 CE) and modern nutritional science paradigms, supporting the translational validity of Yogic dietary interventions in geriatric care.
Table 5. The Panchakosha-Nutritional Integration Model: Mapping Classical Yogic Constructs onto Modern Nutritional Science Domains
| Kosha (Sheath) | Sanskrit meaning | Nutritional domain | Yogic dietary practice | Modern scientific correlate |
| Annamaya Kosha | Physical / food body | Macronutrient adequacy; body composition | Sattvic Ahar; Mitahara (portion control) | Protein-energy sufficiency; BMI; anthropometrics |
| Pranamaya Kosha | Vital / energetic body | Metabolic energy; micronutrient status | Shadrasatmak Ahar (six-taste diversity); Bhojan Kala | Metabolic rate; micronutrient panels; circadian nutrition |
| Manomaya Kosha | Mental / emotional body | Mood, cognition, psychological well-being | Avoidance of Rajasic and Tamasic foods; mindful eating | Dietary psychiatry; gut-brain axis; neuroinflammation |
| Vijnanamaya Kosha | Wisdom / discriminative body | Health literacy; self-regulatory capacity | Conscious food selection; dietary education | Self-efficacy in nutrition; behavioral nutrition science |
| Anandamaya Kosha | Bliss / causal body | Subjective well-being; quality of life | Integration of Yoga, meditation, and Sattvic diet | Positive psychology; hedonic and eudaimonic well-being |
Figure 3. The Panchakosha-Nutritional Integration Model. Concentric circles representing the five Koshas (sheaths) of the Yogic framework, from innermost (Annamaya Kosha: physical nutrition) to outermost (Anandamaya Kosha: bliss/well-being), each mapped to its corresponding modern nutritional science domain. The model provides a theoretical basis for holistic, multi-dimensional nutritional assessment in older adults.
The clinical significance of these findings merits explicit statement. A shift from “at-risk” to “normal” nutritional status on the MNA corresponds to a clinically meaningful reduction in adverse health outcomes: prior literature estimates that correcting malnutrition risk in community-dwelling elderly is associated with an approximately 30–40% reduction in unplanned hospitalization risk, a significant reduction in length of hospital stay, and measurable improvements in functional capacity and quality of life (36, 37). In the Indian public health context, where nutritional education interventions are scalable at low cost through community health worker networks, the number needed to treat of approximately 11 (28) implies that for every 11 elderly individuals receiving a structured nutritional education program (37), one additional person is moved from malnutrition risk to normal nutritional status — a clinically and economically meaningful outcome at population scale (38).
The improvements in appetite observed across included studies are biologically plausible (39). The Sattvic dietary framework incorporates specific culinary spices, cumin, ginger, fennel, coriander, and turmeric, that carry well-documented appetitive, carminative, and anti-inflammatory properties (40). Ginger, for instance, has been shown to accelerate gastric emptying and attenuate nausea, effects that may be particularly relevant for older adults in whom delayed gastric emptying contributes to early satiety and inadequate caloric intake (41). The systematic inclusion of such spices within the Sattvic dietary protocol, far from being merely ceremonial, represents a nutritionally functional strategy with mechanistically coherent physiological effects.
The improvements in bowel function across studies are consistent with the well-established role of dietary fibre in promoting gastrointestinal motility, stool consistency, and microbiome diversity (33). Constipation affects up to 40% of community-dwelling older adults and is closely linked to reduced appetite, abdominal discomfort, and diminished quality of life (42). The Sattvic dietary protocol emphasizes whole grains, seasonal fruits, legumes, and vegetables, delivering a dietary fibre intake substantially higher than that typically consumed by sedentary older adults, providing a plausible mechanism for the bowel function improvements observed.
The association between the Sattvic dietary pattern and improved sleep quality warrants particular attention, as it represents perhaps the most novel and theoretically interesting finding of this review. Sleep disturbance in older adults is multifactorial and pharmacologically challenging to manage, with available treatments carrying significant adverse effect profiles in this population (43). The mechanisms by which a Sattvic diet may improve sleep are likely multidimensional. Nutritionally, whole grains, dairy products, and legumes, cornerstones of the Sattvic food pattern, are rich in tryptophan, the dietary precursor to both serotonin and melatonin, key regulators of sleep-wake architecture (44). The Bhojan Kala principle of early dinner timing, by reducing nocturnal gastrointestinal activity and its associated sleep-disrupting effects, provides a behavioral complement to these nutritional mechanisms. The elimination of Rajasic stimulants (caffeine-containing beverages and heavily spiced foods consumed in the evening) further contributes to sleep-promoting conditions. Collectively, these mechanisms position the Sattvic dietary pattern as a potentially valuable non-pharmacological approach to sleep management in elderly populations, an application that merits dedicated investigation in future research.
The novel Panchakosha-Nutritional Integration Model proposed in this review represents a theoretical advance beyond previous descriptions of Yogic dietary philosophy in the nutritional literature. Prior work has largely treated Yogic dietary principles descriptively, as objects of historical or anthropological interest, rather than as a structured conceptual framework capable of generating testable hypotheses and guiding outcome selection in empirical research. By mapping the five Koshas onto five corresponding domains of modern nutritional science, namely physical, metabolic, psycho-emotional, cognitive, and eudaimonic well-being, the proposed model provides a systematic architecture for holistic assessment of Yogic dietary interventions that transcends the limitations of reductive, single-outcome study designs. This framework may also prove valuable for researchers working at the intersection of integrative medicine, positive psychology, and geriatric nutrition.
Study limitations and strengths
Several limitations of the available evidence must be explicitly acknowledged. The body of eligible empirical studies is small. Sample sizes are modest, and most studies lack the methodological rigour of adequately powered randomized designs with blinded outcome assessment. The reliance on self-reported secondary outcomes (appetite, bowel function, sleep quality) introduces the possibility of social desirability bias. The absence of biochemical nutritional markers, serum albumin, pre-albumin, haemoglobin, micronutrient concentrations, across most studies precludes mechanistic interpretation of the observed nutritional improvements and limits the assessment of their clinical depth. Dietary adherence was monitored primarily through interview and family corroboration in the clinical studies, without objective biomarkers of intake. Adherence rates were not uniformly reported across studies; where reported Karthikeyan et al. 2021 (27), adherence was noted as high (> 85%) based on session attendance records, though the absence of standardized adherence measurement across studies limits cross-study comparability. For future studies, adequate adherence is recommended to be defined as completion of ≥ 80% of prescribed dietary sessions or meal logs; this threshold was not uniformly defined or reported across the included studies. The heterogeneity of intervention protocols across studies, differing in dietary components, duration, delivery mode, and adherence monitoring strategies, further constrains cross-study comparison. Publication bias is an acknowledged limitation of this review: with only six included empirical studies, formal publication bias assessment using funnel plot analysis or Egger’s test is not statistically feasible (a minimum of ten studies is required for such analyses). It is plausible that studies reporting null or negative effects of Yogic and traditional dietary interventions may have been less likely to be published, particularly in regional and grey literature sources, potentially resulting in an overestimation of intervention effects. This caveat should be considered when interpreting the review findings. Additionally, the review protocol was retrospectively registered on the Open Science Framework (OSF;https://osf.io/r42h5/overview?view_only=8aa7c085416e4e4f92265c33656ad90c) following completion of data extraction. While prospective registration in PROSPERO would have been preferable, the retrospective OSF registration provides a time-stamped record of the review protocol and mitigates, in part, the risk of selective outcome reporting bias.
This review has several notable strengths:
The improvements in appetite observed across included studies are biologically plausible (39). The Sattvic dietary framework incorporates specific culinary spices, cumin, ginger, fennel, coriander, and turmeric, that carry well-documented appetitive, carminative, and anti-inflammatory properties (40). Ginger, for instance, has been shown to accelerate gastric emptying and attenuate nausea, effects that may be particularly relevant for older adults in whom delayed gastric emptying contributes to early satiety and inadequate caloric intake (41). The systematic inclusion of such spices within the Sattvic dietary protocol, far from being merely ceremonial, represents a nutritionally functional strategy with mechanistically coherent physiological effects.
The improvements in bowel function across studies are consistent with the well-established role of dietary fibre in promoting gastrointestinal motility, stool consistency, and microbiome diversity (33). Constipation affects up to 40% of community-dwelling older adults and is closely linked to reduced appetite, abdominal discomfort, and diminished quality of life (42). The Sattvic dietary protocol emphasizes whole grains, seasonal fruits, legumes, and vegetables, delivering a dietary fibre intake substantially higher than that typically consumed by sedentary older adults, providing a plausible mechanism for the bowel function improvements observed.
The association between the Sattvic dietary pattern and improved sleep quality warrants particular attention, as it represents perhaps the most novel and theoretically interesting finding of this review. Sleep disturbance in older adults is multifactorial and pharmacologically challenging to manage, with available treatments carrying significant adverse effect profiles in this population (43). The mechanisms by which a Sattvic diet may improve sleep are likely multidimensional. Nutritionally, whole grains, dairy products, and legumes, cornerstones of the Sattvic food pattern, are rich in tryptophan, the dietary precursor to both serotonin and melatonin, key regulators of sleep-wake architecture (44). The Bhojan Kala principle of early dinner timing, by reducing nocturnal gastrointestinal activity and its associated sleep-disrupting effects, provides a behavioral complement to these nutritional mechanisms. The elimination of Rajasic stimulants (caffeine-containing beverages and heavily spiced foods consumed in the evening) further contributes to sleep-promoting conditions. Collectively, these mechanisms position the Sattvic dietary pattern as a potentially valuable non-pharmacological approach to sleep management in elderly populations, an application that merits dedicated investigation in future research.
The novel Panchakosha-Nutritional Integration Model proposed in this review represents a theoretical advance beyond previous descriptions of Yogic dietary philosophy in the nutritional literature. Prior work has largely treated Yogic dietary principles descriptively, as objects of historical or anthropological interest, rather than as a structured conceptual framework capable of generating testable hypotheses and guiding outcome selection in empirical research. By mapping the five Koshas onto five corresponding domains of modern nutritional science, namely physical, metabolic, psycho-emotional, cognitive, and eudaimonic well-being, the proposed model provides a systematic architecture for holistic assessment of Yogic dietary interventions that transcends the limitations of reductive, single-outcome study designs. This framework may also prove valuable for researchers working at the intersection of integrative medicine, positive psychology, and geriatric nutrition.
Study limitations and strengths
Several limitations of the available evidence must be explicitly acknowledged. The body of eligible empirical studies is small. Sample sizes are modest, and most studies lack the methodological rigour of adequately powered randomized designs with blinded outcome assessment. The reliance on self-reported secondary outcomes (appetite, bowel function, sleep quality) introduces the possibility of social desirability bias. The absence of biochemical nutritional markers, serum albumin, pre-albumin, haemoglobin, micronutrient concentrations, across most studies precludes mechanistic interpretation of the observed nutritional improvements and limits the assessment of their clinical depth. Dietary adherence was monitored primarily through interview and family corroboration in the clinical studies, without objective biomarkers of intake. Adherence rates were not uniformly reported across studies; where reported Karthikeyan et al. 2021 (27), adherence was noted as high (> 85%) based on session attendance records, though the absence of standardized adherence measurement across studies limits cross-study comparability. For future studies, adequate adherence is recommended to be defined as completion of ≥ 80% of prescribed dietary sessions or meal logs; this threshold was not uniformly defined or reported across the included studies. The heterogeneity of intervention protocols across studies, differing in dietary components, duration, delivery mode, and adherence monitoring strategies, further constrains cross-study comparison. Publication bias is an acknowledged limitation of this review: with only six included empirical studies, formal publication bias assessment using funnel plot analysis or Egger’s test is not statistically feasible (a minimum of ten studies is required for such analyses). It is plausible that studies reporting null or negative effects of Yogic and traditional dietary interventions may have been less likely to be published, particularly in regional and grey literature sources, potentially resulting in an overestimation of intervention effects. This caveat should be considered when interpreting the review findings. Additionally, the review protocol was retrospectively registered on the Open Science Framework (OSF;https://osf.io/r42h5/overview?view_only=8aa7c085416e4e4f92265c33656ad90c) following completion of data extraction. While prospective registration in PROSPERO would have been preferable, the retrospective OSF registration provides a time-stamped record of the review protocol and mitigates, in part, the risk of selective outcome reporting bias.
This review has several notable strengths:
- First systematic synthesis of Yogic and Ayurvedic dietary interventions in geriatric populations, addressing a recognized gap in the evidence base for traditional Indian nutritional medicine.
- Inclusion of classical primary textual sources (Bhagavad Gita (13), Hatha Yoga Pradipika (14), Gherand Samhita (29), Charak Samhita (21)) alongside empirical evidence, providing a uniquely integrated theoretical-empirical framework.
- Novel Panchakosha-Nutritional Integration Model as a theoretical contribution, offering a structured mapping of classical Yogic constructs onto modern nutritional science domains with direct clinical applicability.
- Rigorous adherence to PRISMA 2020 reporting guidelines, with all noted methodological exceptions explicitly acknowledged as limitations.
- Comprehensive search across eight databases including Indian-specific repositories (IAMJ, IndMED, Cureus) alongside major international databases, with search strategy documented in Appendix S1.
Conclusion
This systematic review consolidates the available evidence indicating that Yogic dietary interventions, grounded in the classical principles of Sattvic Ahar, Mitahara, Bhojan Kala, and Ayurvedic nutritional philosophy, are associated with meaningful improvements in nutritional status, appetite, bowel function, and sleep quality in community-dwelling older adults. The body of evidence, though still modest, is directionally consistent and theoretically coherent, supported by a philosophical framework that aligns substantively with contemporary nutritional science across multiple domains.
The Panchakosha-Nutritional Integration Model introduced in this review offers a novel conceptual bridge between the Yogic epistemological tradition and modern nutritional science. By organizing the multidimensional health impacts of Yogic dietary practice within a coherent and testable five-domain framework, this model has the potential to enrich the theoretical grounding of future research and to expand the scope of outcome measurement beyond conventional anthropometric and biochemical endpoints toward a more holistic understanding of nutritional well-being in older adults.
The principles of Yogic diet, which emphasize whole foods, plant predominance, mindful preparation and consumption, seasonal attunement, and portion consciousness, are not merely culturally specific practices. They represent a distillation of dietary wisdom that is, as this review demonstrates, substantively convergent with the most robust evidence-based dietary recommendations available to contemporary science. Their accessibility, cultural resonance, and low-cost nature make them particularly well-suited for deployment as public health interventions in the large and rapidly aging populations of South Asia and its diaspora.
Future research should prioritize adequately powered, multi-center randomized controlled trials with clearly specified and replicable Yogic dietary protocols, extended follow-up periods, and comprehensive biochemical and functional outcome assessments. Studies examining the additive effects of combining Yogic dietary practice with other components of the Yoga system (including asana (45), pranayama, and meditation) on nutritional and functional outcomes in older adults represent a particularly promising and currently underexplored direction. The integration of the Panchakosha framework into the design and reporting of such trials would represent a meaningful step toward a more holistic and scientifically credible evidence base for Yogic approaches to healthy aging.
The Panchakosha-Nutritional Integration Model introduced in this review offers a novel conceptual bridge between the Yogic epistemological tradition and modern nutritional science. By organizing the multidimensional health impacts of Yogic dietary practice within a coherent and testable five-domain framework, this model has the potential to enrich the theoretical grounding of future research and to expand the scope of outcome measurement beyond conventional anthropometric and biochemical endpoints toward a more holistic understanding of nutritional well-being in older adults.
The principles of Yogic diet, which emphasize whole foods, plant predominance, mindful preparation and consumption, seasonal attunement, and portion consciousness, are not merely culturally specific practices. They represent a distillation of dietary wisdom that is, as this review demonstrates, substantively convergent with the most robust evidence-based dietary recommendations available to contemporary science. Their accessibility, cultural resonance, and low-cost nature make them particularly well-suited for deployment as public health interventions in the large and rapidly aging populations of South Asia and its diaspora.
Future research should prioritize adequately powered, multi-center randomized controlled trials with clearly specified and replicable Yogic dietary protocols, extended follow-up periods, and comprehensive biochemical and functional outcome assessments. Studies examining the additive effects of combining Yogic dietary practice with other components of the Yoga system (including asana (45), pranayama, and meditation) on nutritional and functional outcomes in older adults represent a particularly promising and currently underexplored direction. The integration of the Panchakosha framework into the design and reporting of such trials would represent a meaningful step toward a more holistic and scientifically credible evidence base for Yogic approaches to healthy aging.
Ethical approval and consent to participate
Not applicable (systematic review of previously published studies; no human subjects were directly involved).
Conflict of interest
The author declares no conflict of interest.
Acknowledgements
The author gratefully acknowledges the scholars and practitioners of Yoga and Ayurveda whose foundational contributions underpin the theoretical framework of this review, the researchers whose empirical work is synthesized herein, and the elderly participants in the included studies for their willingness to contribute to this field of inquiry.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization, systematic search strategy, data extraction, quality assessment, narrative synthesis, original model development (Panchakosha-Nutritional Integration Model), writing (original draft), review, editing, and final approval of the manuscript.
References
- World Health Organization. Ageing and health [Internet]. 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health
- Lochs H, Allison SP, Meier R, Pirlich M, Kondrup J, Schneider ST, et al. Introductory to the ESPEN Guidelines on enteral nutrition: terminology, definitions and general topics. Clinical Nutrition. 2006; 25(2): 180-6.
- White JV, Guenter P, Jensen G, Malone A, Schofield M. Consensus statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: characteristics recommended for the identification and documentation of adult malnutrition. Journal of Parenteral and Enteral Nutrition. 2012; 36(3): 275-83.
- Agarwal E, Miller M, Yaxley A, Isenring E. Malnutrition in the elderly: a narrative review. Maturitas. 2013; 76(4): 296-302.
- Rasheed S, Woods RT. Malnutrition and quality of life in older people: a systematic review and meta-analysis. Ageing Research Reviews. 2013; 12(2): 561-6.
- Sullivan DH, Bopp MM, Roberson PK. Protein-energy undernutrition and life-threatening complications among the hospitalized elderly. Journal of General Internal Medicine. 2002; 17(12): 923-32.
- Govindaraju T, Owen AJ, McCaffrey TA. Past, present and future influences of diet among older adults -- a scoping review. Ageing Research Review. 2022; 77: 101600.
- Morley JE. Undernutrition in older adults. Family Practice. 2012; 29(Suppl 1): 89-93.
- Neumann SA, Miller MD, Daniels L, Crotty M. Nutritional status and clinical outcomes of older patients in rehabilitation. Journal of Human and Nutrition and Dietetics. 2005; 18(2): 129-36.
- Firth J, Gangwisch JE, Borsini A, Wootton RE, Mayer EA. Food and mood: how do diet and nutrition affect mental wellbeing? BMJ. 2020; 369: 2382.
- Opie RS, Itsiopoulos C, Parletta N, Sanchez-Villegas A, Akbaraly TN, Ruusunen A. Dietary recommendations for the prevention of depression. Nutritional Neuroscience. 2017; 20(3): 161-71.
- Kris-Etherton PM, Petersen KS, Hibbeln JR, Hurley D, Kolick V, Peoples S. Nutrition and behavioral health disorders: depression and anxiety. Nutrition Reviews. 2021; 79(3): 247-60.
- Chapple CK, editor. The Bhagavad Gita [Sargeant W, trans]. 25th anniversary ed. Albany: State University of New York Press; 2009. Chap. 17, P. 7-10.
- Muktibodhananda S. The Hatha Yoga Pradipika [Akers BD, trans]. Woodstock: YogaVidya.com; 2002. Chap. 1, P. 59-63.
- Mallinson J. The shiva samhita: a critical edition and an English translation. Woodstock: YogaVidya.com; 2007. Chap. 3, P. 33-39.
- Chordia N. Concept of yogic diet according to yoga literature. International Journal of Physiology, Nutrition and Physical Education Sports Health. 2018; 3(2): 2255-57.
- Sharma A. Sushrut Samhita of Sushrut, Chikitsasthan. Chap. 24, Verse 68. Varanasi: Choukhamba Surbharti Prakashan; 2015: 362.
- Shrilakshmipatishastri V. Vidyotini Hindi Tika on Yogratnakar, Nityapravruttiprakar. Varanasi: Choukhamba Prakashan; 2021. P. 140.
- Leitzmann C. Vegetarian diets: what are the advantages? Forum of Nutrition. 2005; 57: 147-56.
- Flanagan A, Bechtold DA, Pot GK, Johnston JD. Chrono-nutrition: from molecular and neuronal mechanisms to human epidemiology and timed feeding patterns. Journal of Neurochemistry. 2021; 157(1): 53-72.
- Agnivesha. Charaka Samhita (revised by Charaka and Dridhabala), with Ayurveda Dipika commentary by Chakrapanidatta, ed. Yadavji Trikamji Acharya. Varanasi: Chaukhamba Sanskrit Sansthan; 2016.
- Shuremu M, Hassen Abate K, Belachew T. Effect of nutrition education intervention to improve dietary diversity practice and nutritional status of the older people: A cluster randomized controlled trial. Food Science & Nutrition. 2023; 11(10): 6071–83.
- Carcelén-Fraile MC, Martín-Baute MR, Ledesma-Cerrato MI, Castellote-Caballero Y, González-Martín AM, Hita-Contreras F, et al. Effects of a yoga program combined with a Mediterranean diet on nutritional status and functional capacity in community-dwelling older adults: A randomized controlled clinical trial. Nutrients. 2024; 16(11): 1601.
- Koren-Hakim T, Weiss A, Hershkovitz A, Otzrateni I, Anbar R, Gross Nevo RF, et al. Comparing the adequacy of the MNA-SF, NRS-2002 and MUST nutritional tools in assessing malnutrition in hip fracture operated elderly patients. Clinical Nutrition. 2016; 35(5): 1053-8.
- Krishnamoorthy Y, Vijayageetha M, Saya GK. Validation and reliability assessment of the Mini-Nutritional Assessment–Short Form questionnaire among older adults in South India. Indian Journal of Community Medicine. 2021; 46(1): 70–4.
- Shalini T, Chitra PS, Naveen Kumar B, Madhavi G, Bhanuprakash Reddy G. Frailty and nutritional status among urban older adults in South India. Journal of Aging Research. 2020; 2020: 1-11.
- Karthikeyan MS, Vijaykumar P, Chandana L, Paul AB. Impact of nutritional education in malnourished elderly patients with the comparison of mini nutritional assessment (MNA) score. Journal of Family Medicine and Primary Care. 2021; 10(3): 1167–70.
- Meena JJ, Singh A, Gupta N, Meena GS. Effect of health education on nutritional status of elderly population in a rural area in Delhi: An interventional study. Cureus. 2025; 17(5): 1-8.
- The Gheranda Samhita: the original Sanskrit and an English translation [Mallinson J, trans]. Woodstock: YogaVidya.com; 2004. Chap. 5, P. 16-21.
- Manoogian ENC, Chaix A, Panda S. When to eat: the importance of eating patterns in health and disease. Journal of Biological Rhythms. 2019; 34(6): 579-81.
- Fontana L, Partridge L, Longo VD. Extending healthy life span -- from yeast to humans. Science. 2010; 328(5976): 321-6.
- Longo VD, Anderson RM. Nutrition, longevity and disease: from molecular mechanisms to interventions. Cell. 2022; 185(9): 1455-70.
- Dahl WJ, Zhu H, Guan G, Telle-Hansen VH. Dietary fibre, gut microbiota and metabolic regulation -- current status in human randomised trials. Nutrients. 2023; 15(9): 1-18.
- Cryan JF, O'Riordan KJ, Cowan CSM, Sandhu KV, Bastiaanssen TFS, Boehme M, et al. The microbiota-gut-brain axis. Physiological Reviews. 2019; 99(4): 1877-2013.
- Lane MM, Gamage E, Travica N, Dissanayaka T, Ashtree DN, Gauci S, et al. Ultra-processed food consumption and mental health: A systematic review and meta-analysis of observational studies. Nutrients. 2022; 14(13): 1-22.
- Valmorbida E, Trevisan C, Imoscopi A, Mazzochin M, Manzato E, Sergi G. Malnutrition is associated with increased risk of hospital admission and death in the first 18 months of institutionalization. Clinical Nutrition. 2020; 39(12): 3687-94.
- Fernandez-Barres S, Garcia-Barco M, Basora J, Martínez T, Pedret R, Arija V, et al The efficacy of a nutrition education intervention to prevent risk of malnutrition for dependent elderly patients receiving Home Care: A randomized controlled trial. International Jourmal of Nursing Studies. 2017; 70: 131-41.
- Gomez G, Botero-Rodriguez F, Misas JD, Garcia-Cifuentes E, Sulo S, Brunton C, et al. A nutritionally focused program for community-living older adults was associated with improved health and well-being. Clinical Nutrition. 2022; 41(7): 1549-56.
- Morley JE, Miller DK, Perry HM, Patrick P, Guigoz Y, Vellas B. Anorexia of aging, leptin, and the Mini Nutritional Assessment. Nestle Nutrition Workshop Series: Clinical & Performance Programme. 1999; 1: 67-76.
- Tapsell LC, Hemphill I, Cobiac L, Patch CS, Sullivan DR, Fenech M, et al. Health benefits of herbs and spices: the past, the present, the future. The Medical Journal of Australia. 2006; 185(S4): 1–24.
- Wu KL, Rayner CK, Chuah SK, Changchien CS, Lu SN, Chiu YC, et al. Effects of ginger on gastric emptying and motility in healthy humans. Europen Journal of Gastroenterology & Hepatology. 2008; 20(5): 436-40.
- Rao SSC, Rattanakovit K, Patcharatrakul T. Diagnosis and management of chronic constipation in adults. Nature Reviews, Gastroenterology & Hepatology. 2016; 13(5): 295-305.
- Bloom HG, Ahmed I, Alessi CA, Ancoli-Israel S, Buysse DJ, Kryger MH, et al. Evidence-based recommendations for the assessment and management of sleep disorders in older persons. Journal of the American Geriatrics Society. 2009; 57(5): 761-89.
- Peuhkuri K, Sihvola N, Korpela R. Diet promotes sleep duration and quality. Nutrition Research. 2012; 32(5): 309-19.
- Iyengar BKS. Light on Yoga. London: HarperCollins; 2005.
Type of Study: Applicable |
Subject:
General
Received: 2026/05/3 | Accepted: 2026/06/14 | Published: 2026/06/20
Received: 2026/05/3 | Accepted: 2026/06/14 | Published: 2026/06/20
References
1. World Health Organization. Ageing and health [Internet]. 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health
2. Lochs H, Allison SP, Meier R, Pirlich M, Kondrup J, Schneider ST, et al. Introductory to the ESPEN Guidelines on enteral nutrition: terminology, definitions and general topics. Clinical Nutrition. 2006; 25(2): 180-6.
3. White JV, Guenter P, Jensen G, Malone A, Schofield M. Consensus statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: characteristics recommended for the identification and documentation of adult malnutrition. Journal of Parenteral and Enteral Nutrition. 2012; 36(3): 275-83.
4. Agarwal E, Miller M, Yaxley A, Isenring E. Malnutrition in the elderly: a narrative review. Maturitas. 2013; 76(4): 296-302.
5. Rasheed S, Woods RT. Malnutrition and quality of life in older people: a systematic review and meta-analysis. Ageing Research Reviews. 2013; 12(2): 561-6.
6. Sullivan DH, Bopp MM, Roberson PK. Protein-energy undernutrition and life-threatening complications among the hospitalized elderly. Journal of General Internal Medicine. 2002; 17(12): 923-32.
7. Govindaraju T, Owen AJ, McCaffrey TA. Past, present and future influences of diet among older adults -- a scoping review. Ageing Research Review. 2022; 77: 101600.
8. Morley JE. Undernutrition in older adults. Family Practice. 2012; 29(Suppl 1): 89-93.
9. Neumann SA, Miller MD, Daniels L, Crotty M. Nutritional status and clinical outcomes of older patients in rehabilitation. Journal of Human and Nutrition and Dietetics. 2005; 18(2): 129-36.
10. Firth J, Gangwisch JE, Borsini A, Wootton RE, Mayer EA. Food and mood: how do diet and nutrition affect mental wellbeing? BMJ. 2020; 369: 2382.
11. Opie RS, Itsiopoulos C, Parletta N, Sanchez-Villegas A, Akbaraly TN, Ruusunen A. Dietary recommendations for the prevention of depression. Nutritional Neuroscience. 2017; 20(3): 161-71.
12. Kris-Etherton PM, Petersen KS, Hibbeln JR, Hurley D, Kolick V, Peoples S. Nutrition and behavioral health disorders: depression and anxiety. Nutrition Reviews. 2021; 79(3): 247-60.
13. Chapple CK, editor. The Bhagavad Gita [Sargeant W, trans]. 25th anniversary ed. Albany: State University of New York Press; 2009. Chap. 17, P. 7-10.
14. Muktibodhananda S. The Hatha Yoga Pradipika [Akers BD, trans]. Woodstock: YogaVidya.com; 2002. Chap. 1, P. 59-63.
15. Mallinson J. The shiva samhita: a critical edition and an English translation. Woodstock: YogaVidya.com; 2007. Chap. 3, P. 33-39.
16. Chordia N. Concept of yogic diet according to yoga literature. International Journal of Physiology, Nutrition and Physical Education Sports Health. 2018; 3(2): 2255-57.
17. Sharma A. Sushrut Samhita of Sushrut, Chikitsasthan. Chap. 24, Verse 68. Varanasi: Choukhamba Surbharti Prakashan; 2015: 362.
18. Shrilakshmipatishastri V. Vidyotini Hindi Tika on Yogratnakar, Nityapravruttiprakar. Varanasi: Choukhamba Prakashan; 2021. P. 140.
19. Leitzmann C. Vegetarian diets: what are the advantages? Forum of Nutrition. 2005; 57: 147-56.
20. Flanagan A, Bechtold DA, Pot GK, Johnston JD. Chrono-nutrition: from molecular and neuronal mechanisms to human epidemiology and timed feeding patterns. Journal of Neurochemistry. 2021; 157(1): 53-72.
21. Agnivesha. Charaka Samhita (revised by Charaka and Dridhabala), with Ayurveda Dipika commentary by Chakrapanidatta, ed. Yadavji Trikamji Acharya. Varanasi: Chaukhamba Sanskrit Sansthan; 2016.
22. Shuremu M, Hassen Abate K, Belachew T. Effect of nutrition education intervention to improve dietary diversity practice and nutritional status of the older people: A cluster randomized controlled trial. Food Science & Nutrition. 2023; 11(10): 6071–83.
23. Carcelén-Fraile MC, Martín-Baute MR, Ledesma-Cerrato MI, Castellote-Caballero Y, González-Martín AM, Hita-Contreras F, et al. Effects of a yoga program combined with a Mediterranean diet on nutritional status and functional capacity in community-dwelling older adults: A randomized controlled clinical trial. Nutrients. 2024; 16(11): 1601.
24. Koren-Hakim T, Weiss A, Hershkovitz A, Otzrateni I, Anbar R, Gross Nevo RF, et al. Comparing the adequacy of the MNA-SF, NRS-2002 and MUST nutritional tools in assessing malnutrition in hip fracture operated elderly patients. Clinical Nutrition. 2016; 35(5): 1053-8.
25. Krishnamoorthy Y, Vijayageetha M, Saya GK. Validation and reliability assessment of the Mini-Nutritional Assessment–Short Form questionnaire among older adults in South India. Indian Journal of Community Medicine. 2021; 46(1): 70–4.
26. Shalini T, Chitra PS, Naveen Kumar B, Madhavi G, Bhanuprakash Reddy G. Frailty and nutritional status among urban older adults in South India. Journal of Aging Research. 2020; 2020: 1-11.
27. Karthikeyan MS, Vijaykumar P, Chandana L, Paul AB. Impact of nutritional education in malnourished elderly patients with the comparison of mini nutritional assessment (MNA) score. Journal of Family Medicine and Primary Care. 2021; 10(3): 1167–70.
28. Meena JJ, Singh A, Gupta N, Meena GS. Effect of health education on nutritional status of elderly population in a rural area in Delhi: An interventional study. Cureus. 2025; 17(5): 1-8.
29. The Gheranda Samhita: the original Sanskrit and an English translation [Mallinson J, trans]. Woodstock: YogaVidya.com; 2004. Chap. 5, P. 16-21.
30. Manoogian ENC, Chaix A, Panda S. When to eat: the importance of eating patterns in health and disease. Journal of Biological Rhythms. 2019; 34(6): 579-81.
31. Fontana L, Partridge L, Longo VD. Extending healthy life span -- from yeast to humans. Science. 2010; 328(5976): 321-6.
32. Longo VD, Anderson RM. Nutrition, longevity and disease: from molecular mechanisms to interventions. Cell. 2022; 185(9): 1455-70.
33. Dahl WJ, Zhu H, Guan G, Telle-Hansen VH. Dietary fibre, gut microbiota and metabolic regulation -- current status in human randomised trials. Nutrients. 2023; 15(9): 1-18.
34. Cryan JF, O'Riordan KJ, Cowan CSM, Sandhu KV, Bastiaanssen TFS, Boehme M, et al. The microbiota-gut-brain axis. Physiological Reviews. 2019; 99(4): 1877-2013.
35. Lane MM, Gamage E, Travica N, Dissanayaka T, Ashtree DN, Gauci S, et al. Ultra-processed food consumption and mental health: A systematic review and meta-analysis of observational studies. Nutrients. 2022; 14(13): 1-22.
36. Valmorbida E, Trevisan C, Imoscopi A, Mazzochin M, Manzato E, Sergi G. Malnutrition is associated with increased risk of hospital admission and death in the first 18 months of institutionalization. Clinical Nutrition. 2020; 39(12): 3687-94.
37. Fernandez-Barres S, Garcia-Barco M, Basora J, Martínez T, Pedret R, Arija V, et al The efficacy of a nutrition education intervention to prevent risk of malnutrition for dependent elderly patients receiving Home Care: A randomized controlled trial. International Jourmal of Nursing Studies. 2017; 70: 131-41.
38. Gomez G, Botero-Rodriguez F, Misas JD, Garcia-Cifuentes E, Sulo S, Brunton C, et al. A nutritionally focused program for community-living older adults was associated with improved health and well-being. Clinical Nutrition. 2022; 41(7): 1549-56.
39. Morley JE, Miller DK, Perry HM, Patrick P, Guigoz Y, Vellas B. Anorexia of aging, leptin, and the Mini Nutritional Assessment. Nestle Nutrition Workshop Series: Clinical & Performance Programme. 1999; 1: 67-76.
40. Tapsell LC, Hemphill I, Cobiac L, Patch CS, Sullivan DR, Fenech M, et al. Health benefits of herbs and spices: the past, the present, the future. The Medical Journal of Australia. 2006; 185(S4): 1–24.
41. Wu KL, Rayner CK, Chuah SK, Changchien CS, Lu SN, Chiu YC, et al. Effects of ginger on gastric emptying and motility in healthy humans. Europen Journal of Gastroenterology & Hepatology. 2008; 20(5): 436-40.
42. Rao SSC, Rattanakovit K, Patcharatrakul T. Diagnosis and management of chronic constipation in adults. Nature Reviews, Gastroenterology & Hepatology. 2016; 13(5): 295-305.
43. Bloom HG, Ahmed I, Alessi CA, Ancoli-Israel S, Buysse DJ, Kryger MH, et al. Evidence-based recommendations for the assessment and management of sleep disorders in older persons. Journal of the American Geriatrics Society. 2009; 57(5): 761-89.
44. Peuhkuri K, Sihvola N, Korpela R. Diet promotes sleep duration and quality. Nutrition Research. 2012; 32(5): 309-19.
45. Iyengar BKS. Light on Yoga. London: HarperCollins; 2005
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
